

")








Improving aortic aneurysm detection with artificial intelligence based on chest computed tomography data
- Authors: Solovev A.V.1,2, Vasilev Y.A.1, Sinitsyn V.E.1,3,4, Petraikin A.V.1, Vladzymyrskyy A.V.1, Shulkin I.M.1, Sharova D.E.1, Semenov D.S.1
-
Affiliations:
- Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
- Morozov Children’s Municipal Clinical Hospital
- Clinical City Hospital named after I.V. Davydovsky
- Lomonosov Moscow State University
- Issue: Vol 5, No 1 (2024)
- Pages: 29-40
- Section: Original Study Articles
- Submitted: 19.09.2023
- Accepted: 19.12.2023
- Published: 19.04.2024
- URL: https://jdigitaldiagnostics.com/DD/article/view/569388
- DOI: https://doi.org/10.17816/DD569388
- ID: 569388

Cite item

Abstract
BACKGROUND: Aortic aneurysms are known as “silent killers” because this potentially fatal condition can be asymptomatic. The annual incidence of thoracic aortic aneurysms and ruptures is approximately 10 and 1.6 per 100,000 individuals, respectively. The mortality rate for ruptured aneurysms ranges from 94% to 100%. Early diagnosis and treatment can be life-saving. Artificial intelligence technologies can significantly improve diagnostic accuracy and save the lives of patients with thoracic aortic aneurysms.
AIM: This study aimed to assess the efficacy of artificial intelligence technologies for detecting thoracic aortic aneurysms on chest computed tomography scans, as well as the possibility of using artificial intelligence as a clinical decision support system for radiologists during the primary interpretation of radiological images.
MATERIALS AND METHODS: The results of using artificial intelligence technologies for detecting thoracic aortic aneurysms on non-contrast chest computed tomography scans were evaluated. A sample of 84,405 patients >18 years old was generated, with 86 cases of suspected thoracic aortic aneurysms based on artificial intelligence data selected and retrospectively assessed by radiologists and vascular surgeons. To assess the age distribution of the aortic diameter, an additional sample of 968 cases was randomly selected from the total number.
RESULTS: In 44 cases, aneurysms were initially identified by radiologists, whereas in 31 cases, aneurysms were not detected initially; however, artificial intelligence aided in their detection. Six studies were excluded, and five studies had false-positive results. Artificial intelligence aids in detecting and highlighting aortic pathological changes in medical images, increasing the detection rate of thoracic aortic aneurysms by 41% when interpreting chest computed tomography scans. The use of artificial intelligence technologies for primary interpretations of radiological studies and retrospective assessments is advisable to prevent underdiagnosis of clinically significant pathologies and improve the detection rate of pathological aortic enlargement. In the additional sample, the incidence of thoracic aortic dilation and thoracic aortic aneurysms in adults was 14.5% and 1.2%, respectively. The findings also revealed an age-dependent diameter of the thoracic aorta in both men and women.
CONCLUSION: The use of artificial intelligence technologies in the primary interpretation of chest computed tomography scans can improve the detection rate of clinically significant pathologies such as thoracic aortic aneurysms. Expanding retrospective screening based on chest computed tomography scans using artificial intelligence can improve the diagnosis of concomitant pathologies and prevent negative consequences.
Full Text
BACKGROUND
According to the World Health Organization, cardiovascular diseases and associated disorders are among the leading causes of death [1]. These diseases include aortic aneurysms, which are known as “silent killers.” They are generally asymptomatic and can result in aortic dissection or rupture, which leads to death in 94%–100% of cases [2, 3]. Very few studies have statistically analyzed the prevalence of thoracic aortic aneurysms [4]. In Russia, the incidence of ascending aortic aneurysms ranges from 0.16% to 1.06%. Notably, a recent large epidemiological study on the incidence of thoracic aortic aneurysms in Russia was performed approximately 40 years ago [5], highlighting the need for further studies.
According to autopsy data collected over 10 years in the Filatov City Clinical Hospital No. 15 (Moscow), a thoracic aortic aneurysm was the cause of death in 0.8% of cases, with aneurysms suspected before death in only 11% of these cases [4]. In the USA, aortic aneurysms are the 17th leading cause of cardiovascular-related death, with an annual prevalence of thoracic aortic aneurysms of approximately 10 per 100,000 of population and an aneurysm rupture prevalence of approximately 1.6 per 100,000 of population [6]. In Sweden, thoracic aneurysms and aortic dissections occur in up to 16.3 per 100,000 of population [7]. According to Yale University data, the annual incidence rates of aneurysm ruptures and aortic dissections are 3.6% and 3.7% of the reported cases, respectively [8].
During screening for lung tumors using chest computed tomography (CT), abnormal thoracic aortic dilatation is detected in up to 8.1% of patients aged >50 years [9, 10].
Opportunistic screening is a prospective and retrospective analysis of relevant cases to identify conditions and risk factors in addition to the target pathology. This strategy eliminates the need for repeated examinations, reducing the patient’s radiation exposure [11].
In 2022, more than 647,000 noncontrasted chest CT studies were performed in Moscow. This number of examinations allows for the opportunistic detection of various pathological conditions, including life-threatening ones such as thoracic aortic dilatation (aneurysm) [12].
Since 2020, the world’s largest study has been conducted in Moscow to assess the efficacy and quality of artificial intelligence (AI) technology: “An experiment on the use of innovative computer vision technologies for the analysis of medical images and further use in the healthcare system of the city of Moscow” (Moscow Experiment) [13]. AI technology is used in the test mode in the Moscow Experiment, under the supervision of experts of the Center for Diagnostics and Telemedicine (Moscow). The process includes a continuous quality assessment of the system and adjustments to its operation, calculations of accuracy metrics, and identification of operation errors and other characteristics. Consequently , conditions are created for performing retrospective studies and processing X-ray findings during the primary analysis by a radiologist.
AIM
To assess the efficacy of AI technology in detecting thoracic aortic aneurysms based on chest CT findings and investigate the possibility of using AI technology as a medical decision support system for radiologists during the primary assessment of X-ray findings.
MATERIALS AND METHODS
Study design
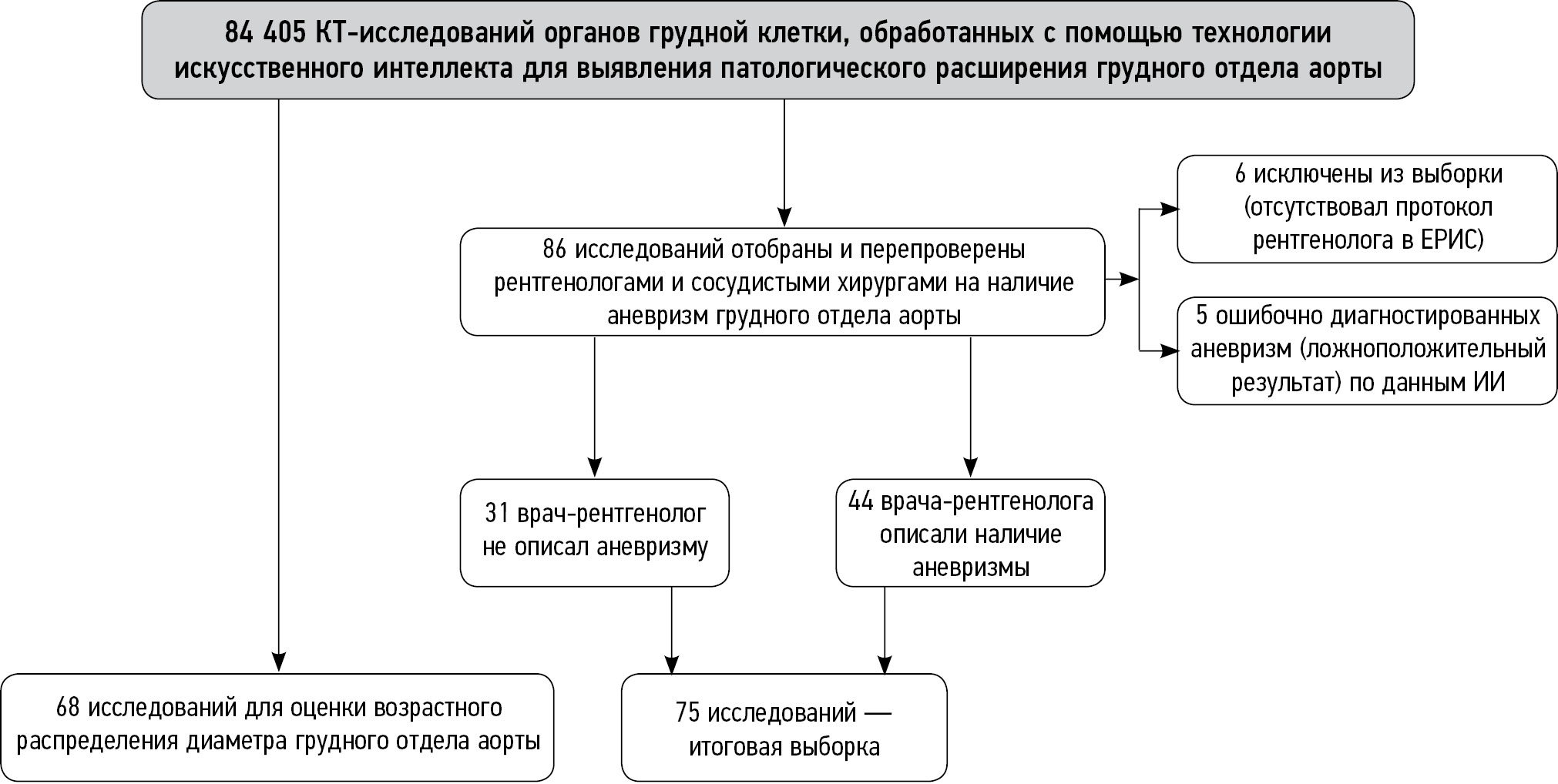
A retrospective analysis of 84,405 chest CT scans was performed. Data were derived from the Unified Radiology Information Service of the automated Unified Medical Information Analysis System (ERIS EMIAS) of Moscow between June 1, 2022, and November 30, 2022, and processed using AI technology. The study design is presented in Fig. 1. The total sample included 84,405 patients aged >18 years, from which 86 examinations with a suspected thoracic aortic aneurysm with a maximum diameter of >50 mm were selected using AI technology data. The examinations were selected by vascular surgeons of the Sklifosovsky Institute for Emergency Medicine.

Fig. 1. Study design. AI, artificial intelligence, CT, computed tomography; ERIS, Unified Radiology Information Service.
The resulting sample was then reviewed by two radiologists from the Center for Diagnostics and Telemedicine with over 5 years of experience. If the first two radiologists disagreed, an expert with 10 years of experience in radiology acted as an arbitrator and made the final decision on the presence of an aneurysm and its description.
During the review, eleven patients were excluded, specifically because the radiologist did not provide a primary protocol in the ERIS in six patients and the results were classified as false positive after AI data processing (assessment of a nontarget pathology or organ) in five patients. The resulting sample included 75 patients referred for a follow-up examination and treatment.
In addition, 1,000 scans were randomly selected from the total sample of 84,405 examinations to assess the distribution of aortic diameter vs. age. After the exclusion of 32 patients due to missing data on patients’ ages, the resulting sample included 968 patients (433 males and 535 females, 44.7% and 55.3%, respectively).
Inclusion criteria
The inclusion criteria for chest CT scans in the sample for analysis using AI technology during the Moscow Experiment in the Thoracic Aortic Aneurysm area were as follows:
- Outpatients and inpatients (male and female patients) of the institutions forming part of the Moscow Healthcare Department (aged >18 years)
- Examination type: noncontrasted chest CT with ≤3 mm slice thickness
- Availability of chest CT scans in the DICOM format and the radiologist’s protocol in the ERIS EMIAS
The exclusion criteria were as follows:
- Patients with surgical hardware (postoperative clamps or plates) creating artifacts in the chest area, including pacemakers
- Contrast enhancement and lung kernel CT
- Absence of chest CT scans in the DICOM format and/or the radiologist’s protocol in the ERIS EMIAS.
Study conditions
According to the basic diagnostic requirements, AI technology was used to process examination findings for detecting abnormal thoracic aortic dilatation. These requirements were developed based on the European Society of Cardiology guidelines on the diagnosis and treatment of aortic diseases [14]:
- Ascending aortic dilatation: 40–49 mm
- Ascending aortic aneurysm: ≥50 mm
- Descending aortic aneurysm: ≥40 mm [15]
The domestic AI algorithm Chest-IRA (IRA Labs, Russia) was used to automatically determine the thoracic aortic diameter. The accuracy of this AI technology was assessed during the Moscow Experiment, with the following results:
- Area under the ROC curve (AUC): 0.99
- Sensitivity: 0.94
- Specificity: 0.96
- Accuracy: 0.95
- Duration of analysis (one examination): 2.1 min [16]
An example of an AI technology algorithm operation is presented in Fig. 2.

Fig. 2. An example of an algorithm operation of a complex AI-based service to process chest CT findings: a: AI technology correctly selected and marked (red line) the suspected ascending and descending thoracic aortic aneurysms; b: a false positive result: a mediastinal neoplasm was marked (red line) together with the ascending thoracic aorta; the green frame indicates the diameter of the descending thoracic aorta. This complex AI-based service has additional modules for marking pulmonary infiltrates (orange outline) and pleural effusion (yellow outline).
The retrospective verification of CT scans with suspected thoracic aortic aneurysms in the total sample of 75 studies (maximum diameter: >50 mm) was performed by two radiologists (with >5 years of experience), one expert radiologist, and vascular surgeons (with >10 years of experience). The correctness of AI technology operation in measuring the thoracic aorta in the axial plane was assessed. According to the guidelines of the European Association of Cardiovascular Imaging and the European Society of Cardiology, the physicians measured both the maximum anteroposterior diameter and the perpendicular diameter of the thoracic aorta [17]. All patients in the sample were referred for a follow-up examination to decide on further monitoring or treatment.
The normality of distribution in the groups of patients was assessed using the Shapiro–Wilk test. Given that the distribution was not normal (p <0.001), all subsample values are presented as median [25th percentile; 75th percentile] and minimum/maximum. Between-group comparisons were performed by the Mann–Whitney method.
RESULTS
Primary study results
The AI technology algorithm was used to process 84,405 noncontrasted chest CT scans for detecting abnormal thoracic aortic dilatation. In total, 86 patients (62 male and 24 female patients) with a suspected thoracic aortic aneurysm according to AI technology findings were selected from this sample and retrospectively reviewed by radiologists and vascular surgeons. Of 86 patients, six were excluded from the sample because no protocol was available in the ERIS, and five had a false positive result after AI data processing (assessment of a nontarget pathology or organ, Fig. 2, b); these five patients were also excluded from the sample.
The resulting sample included 75 patients: 57 male (66 [59; 73]; 27–87 years) and 18 female patients (62 [59; 74]; 47–87 years). Thoracic aortic aneurysms were described in the primary X-ray protocol in 44 (59%) cases; in 31 (41%) cases, aneurysms were not mentioned in the primary protocol. Thus, AI technology allowed for detecting 31 additional cases of thoracic aortic aneurysms (41%). In this group, the maximum thoracic aortic diameter was 56 [54; 60]: 52–84 mm in male and 57 [54; 63]; 52–87 mm in female patients.
Patients with aortic aneurysms detected using AI technology on chest CT scans were informed and referred for follow-up examinations (echocardiography, CT, or magnetic resonance angiography, and cardiologist or vascular surgeon consultation) to determine the management and treatment strategy.
The follow-up examinations provided additional information: 4 (5.33%) of 75 patients died before the end of diagnostic procedures or surgery, and 3 (4%) patients refused follow-up examinations and treatment. Another 31 (41.33%) patients were lost to follow-up.
In 25 (33.33%) of 37 patients who remained under follow-up and continued treatment, thoracic aortic aneurysm was confirmed (ongoing follow-up); in 12 (16%) patients, the diagnosis was clarified (still being treated by a cardiologist). In 3 patients, the diagnosis of aneurysm was not confirmed after a diagnostic examination; these patients were diagnosed with thoracic aortic dilatation. Moreover, two surgeries (aortic stenting) were performed for aneurysms.
No significant differences in age and thoracic aortic diameter were found between the groups of male and female patients with aneurysms detected using AI technology (p>0.05).
Findings of the second part of the study
Preliminary data on the incidence of aneurysms was obtained in the sample including 968 cases (Fig. 3) randomly selected from 84,405 cases. In the adult population (aged ≥18 years), the incidence rates of thoracic aortic dilatation and aneurysms were 14.5% and 1.2%, respectively.

Fig. 3. Plot of the maximum thoracic aortic diameter versus age for the sample including 968 examinations: a: male patients; b: female patients.
The female patients were 65 [51; 75]; 19–102 years old (n = 535), and the male patients were 60 [47; 71]; 18–95 years old (n = 433). There were slightly more female patients than male patients, reflecting the sex distribution in the total patient population studied. The median age of the female patients (65 years) was slightly higher than that of male patients (60 years), and the interquartile ranges were comparable.
In this group, the thoracic aortic diameter was 34 [31; 37]; 20–50 mm in female patients and 36 [33; 39]; 24–60 mm in male patients.
Significant (p<0.001) differences in age and maximum thoracic aortic diameter were found between the male and female patients. A pronounced association of the thoracic aortic diameter and age was found in male and female patients. In male patients, relative age-related changes in the thoracic aortic diameter are more pronounced at 0.177 mm/ year; in female patients, this parameter was 0.118 mm/year.
DISCUSSION
Result summary
The analysis showed no significant differences (p >0.05) in age or maximum thoracic aortic diameter between male and female patients with aortic aneurysms (n = 75). In the sample including 968 patients (randomly selected from the total sample), significant differences (p<0.001) in age and maximum thoracic aortic diameter were found between male and female patients. This highlights the need for age and sex standards to describe the distribution by age. In addition, well-designed studies are necessary for a more comprehensive analysis of the observed trends.
Discussion of study findings
An increase in the detection rate of aneurysms in a retrospective study employing an AI algorithm confirms the efficacy and feasibility of this approach in clinical practice, e.g., as an accessory tool for radiologists during the primary assessment of X-ray findings. However, the software also provided some false positive results. Methods to minimize such errors by monitoring and fine-tuning the algorithm have been reported [20–22].
According to the literature, a positive correlation existed between age and thoracic aortic diameter. Men generally have larger thoracic aortic diameters than women [18], as well as a more pronounced association between age and thoracic aortic diameter [19], which is consistent with the statistical analysis findings in this study.
Physicians are at risk of missing clinically significant conditions for various reasons, including professional burnout (e.g., following the COVID-19 pandemic), increasing workload, and medical personnel shortage. This is another argument in favor of using AI technology as a medical decision support system for radiologists when assessing chest CT scans. AI technology can improve the detection rate and reduce the number of missed clinically significant pathologies [23].
The domestic AI technology used in this study is not the only one in the world, and quality metrics can be used when selecting AI algorithms. Foreign analogs of AI technology are also available for automatic measurement of the thoracic aortic diameter and detection of aneurysms; these solutions allow avoiding errors and can be used in opportunistic screening [24, 25].
According to the literature, AI technology helps radiologists reduce the time spent on detecting pathologies in X-ray images [26, 27].
AI-based solutions are a promising tool for aortic measurements [28]. However, the accuracy of these measurements must be confirmed by further research. This study demonstrates that although AI cannot replace physicians, it can aid radiologists by warning them of potential aortic pathologies, allowing them to avoid missing clinically relevant abnormalities. Radiologists must understand the principle of AI technology operation and possible errors when analyzing study findings [29–33]. Thus, the use of AI in medicine can be a valuable tool in detecting thoracic aortic aneurysms. Accordingly, AI technology must be used to detect abnormal thoracic aortic dilatation during the primary assessment of X-ray findings and in retrospective analysis to reduce the risk of missing clinically significant changes.
CONCLUSIONS
The use of AI technology during the primary assessment of chest CT images and for expanded opportunistic screening may improve the diagnosis of clinically significant pathologies, such as thoracic aortic aneurysms, and prevent unfavorable outcomes. Further optimization of the routing in this patient population requiring urgent medical intervention for timely surgical treatment is crucial. Thus, population reference values for thoracic aortic diameter must be established to adjust the diagnostic criteria for this condition.
ADDITIONAL INFORMATION
Funding source. This article was prepared by the team of authors within the framework of the research work "Opportunistic screening of socially significant and other common diseases" (No. in the Unified State Information System of Accounting: No. 123031400009-1) in accordance with Order of the Department of Health of Moscow from 21.12.2022 No. 1196 "On approval of state tasks, the financial support of which is carried out at the expense of the budget of the city of Moscow state budgetary (autonomous) institutions subordinate to the Department of Health Protection of Moscow, for 2023, 2024 and 2025".
Competing interests. The authors declare that they have no competing interests.
Authors’ contribution. All authors made a substantial contribution to the conception of the work, acquisition, analysis, interpretation of data for the work, drafting and revising the work, final approval of the version to be published and agree to be accountable for all aspects of the work. The major contributions are distributed as follows: A.V. Solovev — research conception and design, article writing, editing, and approval of the final manuscript; Yu.A. Vasilev, V.E. Sinitsyn — research conception, final proofreading of the text; A.V. Petraikin, A.V. Vladzymyrskyy — research conception and design, writing, and editing of the text; I.M. Shulkin, D.E. Sharova, D.S. Semenov — research conception, editing, and approval of the final manuscript, advisory support.
About the authors
Alexander V. Solovev
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies; Morozov Children’s Municipal Clinical Hospital
Email: atlantis.92@mail.ru
ORCID iD: 0000-0003-4485-2638
SPIN-code: 9654-4005
Russian Federation, Moscow; Moscow
Yuriy A. Vasilev
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: VasilevYA1@zdrav.mos.ru
ORCID iD: 0000-0002-0208-5218
SPIN-code: 4458-5608
MD, Cand. Sci. (Medicine)
Russian Federation, MoscowValentin E. Sinitsyn
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies; Clinical City Hospital named after I.V. Davydovsky; Lomonosov Moscow State University
Email: vsini@mail.ru
ORCID iD: 0000-0002-5649-2193
SPIN-code: 8449-6590
MD, Dr. Sci. (Medicine), Professor
Russian Federation, Moscow; Moscow; MoscowAlexey V. Petraikin
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: atlantis.92@mail.ru
ORCID iD: 0000-0003-1694-4682
SPIN-code: 6193-1656
MD, Dr. Sci. (Medicine)
Russian Federation, MoscowAnton V. Vladzymyrskyy
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: VladzimirskijAV@zdrav.mos.ru
ORCID iD: 0000-0002-2990-7736
SPIN-code: 3602-7120
MD, Dr. Sci. (Medicine)
Russian Federation, MoscowIgor M. Shulkin
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: ShulkinIM@zdrav.mos.ru
ORCID iD: 0000-0002-7613-5273
SPIN-code: 5266-0618
Russian Federation, Moscow
Daria E. Sharova
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: SharovaDE@zdrav.mos.ru
ORCID iD: 0000-0001-5792-3912
SPIN-code: 1811-7595
Russian Federation, Moscow
Dmitry S. Semenov
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Author for correspondence.
Email: SemenovDS4@zdrav.mos.ru
ORCID iD: 0000-0002-4293-2514
SPIN-code: 2278-7290
Cand. Sci. (Engineering)
Russian Federation, MoscowReferences
- The top 10 causes of death [Internet]. World Health Organization. [cited 12 May 2023]. Available from: https://www.who.int/ru/news-room/fact-sheets/detail/the-top-10-causes-of-death
- Gouveia e Melo R, Silva Duarte G, Lopes A, et al. Incidence and Prevalence of Thoracic Aortic Aneurysms: A Systematic Review and Meta-analysis of Population-Based Studies. Seminars in thoracic and cardiovascular surgery. 2022;34(1):1–16. doi: 10.1053/j.semtcvs.2021.02.029
- Clinical guidelines. Guidelines for the diagnosis and treatment of aortic diseases (2017). Russian Journal of Cardiology and Cardiovascular Surgery. 2018;11(1):7–67. EDN: YPAKRP
- Kuznechevsky FV, Osipov AKh, Evsikov EM, Abramov IS, Otarova SM. Prevalence and clinical features of aorta aneurysm; and dissections: 10-year results of consequent autopsies made at O.M. Filatov city clinical hospital №15. Russian Journal of Cardiology. 2004;9(6):5–13. EDN: ISVRYL
- Irtyuga OB, Voronkina IV, Smagina LV, et al. The frequency to detect of ascending aorta aneurysms and the mechanism of its development according register of the Almazov Federal Heart, Blood and Endocrinology Centre. Bulletin of Almazov Federal Heart, Blood and Endocrinology Centre. 2011;(5):73–78. EDN: OWGHOB
- Lavall D, Schäfers HJ, Böhm M, Laufs U. Aneurysms of the ascending aorta. Deutsches Arzteblatt international. 2012;109(13):227–233. doi: 10.3238/arztebl.2012.0227
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic Aortic Aneurysm and Dissection. Circulation. 2006;114(24):2611–2618. doi: 10.1161/CIRCULATIONAHA.106.630400
- Elefteriades JA. Natural history of thoracic aortic aneurysms: indications for surgery, and surgical versus nonsurgical risks. The Annals of thoracic surgery. 2002;74(5):1877–1880. doi: 10.1016/s0003-4975(02)04147-4
- Tsai EB, Chiles C, Carter BW, et al. Incidental Findings on Lung Cancer Screening: Significance and Management. Seminars in ultrasound, CT, and MR. 2018;39(3):273–281. doi: 10.1053/j.sult.2018.02.005
- Chernina VYu, Blokhin IA, Nikolaev AE, et al. Tactics for the management of incidentalomas. Section 3. Thyroid, pituitary, vasculature and mediastinum. Moscow: Research and Practical Clinical Center for Diagnostics and Telemedicine; 2019. (In Russ). EDN: WSYSYP
- Law M. “Opportunistic” Screening. J Med Screen. 1994;1(4):208. doi: 10.1177/096914139400100403
- Kumar Y, Hooda K, Li S, et al. Abdominal aortic aneurysm: pictorial review of common appearances and complications. Annals of translational medicine. 2017;5(12):256. doi: 10.21037/atm.2017.04.32
- Vasilev YuA, Vladzymyrskyy AV, editors. Computer Vision in Radiologic Diagnostics: the First Stage of the Moscow Experiment. Moscow: Limited Liability Company Izdatelskie reshenia; 2022. (In Russ). EDN: FOYLXK
- Erbel R, Aboyans V, Boileau C, Vlachopoulos C. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European. European heart journal. 2014;35(41):2873–2926. doi: 10.1093/eurheartj/ehu281
- Documents on the Experiment [Internet]. Center for Diagnostics and Telemedicine. [cited 16 June 2023]. Available from: https://mosmed.ai/ai/docs/
- Chest-IRA [Internet]. Center for Diagnostics and Telemedicine. [cited 16 June 2023]. Available from: https://mosmed.ai/service_catalog/chestira/
- Evangelista A, Sitges M, Jondeau G, et al. Multimodality imaging in thoracic aortic diseases: a clinical consensus statement from the European Association of Cardiovascular Imaging and the European Society of Cardiology working group on aorta and peripheral vascular diseases. European Heart Journal Cardiovascular Imaging. 2023;24(5):e65–e85. doi: 10.1093/ehjci/jead024
- Etli M, Avnioglu S, Yilmaz H, Karahan O. Investigation of the correlation between cardiac parameters and aortic diameter in patients with ascending aortic aneurysm. Egyptian Heart Journal. 2022;74(1):1–7. doi: 10.1186/s43044-022-00238-0
- Pearce W, Slaughter M, Lemaire S, et al. Aortic diameter as a function of age, gender, and body surface area. Surgery. 1993;114(4):691–697.
- Vasilev YA, Bobrovskaya TM, Arzamasov KM, et al. Medical datasets for machine learning: fundamental principles of standartization and systematization. Manager Zdravoohranenia. 2023;4:28–41. EDN: EPGAMD doi: 10.21045/1811-0185-2023-4-28-41
- Chetverikov SF, Arzamasov KM, Andreichenko AE, et al. Approaches to Sampling for Quality Control of Artificial Intelligence in Biomedical Research. Modern Technologies in Medicine. 2023;15(2):19–25. EDN: FUKXYC doi: 10.17691/stm2023.15.2.02
- Zinchenko VV, Arzamasov KM, Chetverikov SF, et al. Methodology for Conducting Post-Marketing Surveillance of Software as a Medical Device Based on Artificial Intelligence Technologies. Modern Technologies in Medicine. 2022;14(5):15–25. doi: 10.17691/stm2022.14.5.02
- Chernina VY, Belyaev MG, Silin AY, et al. A diagnostic and economic evaluation of the complex artificial intelligence algorithm aimed to detect 10 pathologies on the chest CT images. medRxiv. 2023;4. doi: 10.1101/2023.04.19.23288584
- Macruz FBC, Lu C, Strout J, et al. Quantification of the Thoracic Aorta and Detection of Aneurysm at CT: Development and Validation of a Fully Automatic Methodology. Radiology: Artificial Intelligence. 2022;4(2):e210076. doi: 10.1148/ryai.210076
- Adam C, Fabre D, Mougin J, et al. Pre-surgical and Post-surgical Aortic Aneurysm Maximum Diameter Measurement: Full Automation by Artificial Intelligence. European Journal of Vascular and Endovascular Surgery. 2021;62(6):869–877. doi: 10.1016/j.ejvs.2021.07.013
- Vladzymyrskyy AV, Kudryavtsev ND, Kozhikhina DD, et al. Effectiveness of using artificial intelligence technologies for dual descriptions of the results of preventive lung examinations. Profilakticheskaya Meditsina. 2022;25(7):7–15. doi: 10.17116/profmed2022250717
- Rodriguez-Ruiz A, Lång K, Gubern-Merida A, et al. Stand-Alone Artificial Intelligence for Breast Cancer Detection in Mammography: Comparison With 101 Radiologists. Journal of the National Cancer Institute. 2019;111(9):916–922. doi: 10.1093/jnci/djy222
- Rueckel J, Reidler P, Fink N, et al. Artificial intelligence assistance improves reporting efficiency of thoracic aortic aneurysm CT follow-up. European journal of radiology. 2021;134(134):109424. doi: 10.1016/j.ejrad.2020.109424
- Tang A, Tam R, Cadrin-Chênevert A, et al. Canadian Association of Radiologists White Paper on Artificial Intelligence in Radiology. Canadian Association of Radiologists journal. 2018;69(2):120–135. doi: 10.1016/j.carj.2018.02.002
- Certificate of state registration of the database № 2023621046/ 30.03.2023. Vasilev YuA, Turavilova EV, Shul’kin IM, et al. MosMedData: CT scan with signs of abdominal aortic aneurysm. (In Russ). EDN: LXROHZ
- Aliev AF, Kudryavtsev ND, Petraikin AV, et al. Changing of pulmonary artery diameter in accordance with severity of COVID-19 (assessment based on non-contrast computer tomography). Digital Diagnostics. 2021;2(3):249–260. EDN: VTMKCJ doi: 10.17816/DD76726
- Morozov SP, Shapieva AN, Narkevich BYa, et al. Informativity of radial diagnostics methods in various pathological conditions of the organism. Moscow: Research and Practical Clinical Center for Diagnostics and Telemedicine; 2020. (In Russ). EDN: DYEYBT
- Vasilev YuA, Vladzymyrskyy AV, Bondarchuk DV, et al. Importance of artificial intelligence technologies to prevent defects in radiologist’s practice. Medical doctor and IT. 2023;(2):16–27. EDN: SYZAOQ doi: 10.25881/18110193_2023_2_16
Supplementary files

