

")








Possibilities for using the Vimedix 3.2 virtual simulator to train ultrasound specialists
- Authors: Vasilev V.А.1, Kondrichina S.N.1
-
Affiliations:
- Petrozavodsk State University
- Issue: Vol 5, No 1 (2024)
- Pages: 41-52
- Section: Original Study Articles
- Submitted: 20.09.2023
- Accepted: 18.01.2024
- Published: 19.04.2024
- URL: https://jdigitaldiagnostics.com/DD/article/view/586551
- DOI: https://doi.org/10.17816/DD586551
- ID: 586551

Cite item

Abstract
BACKGROUND: In recent years, it has been critical to modify training methods and programs in numerous areas, including ultrasound diagnosis, with the use of various virtual and simulation devices. Because practical experience with employing such technologies in the teaching process is limited, there are few original studies on the subject in Russian and foreign literature.
AIM: To determine the possibilities and algorithms for using a virtual ultrasound simulator to train ultrasound specialists based on the results of related work, as well as to assess the benefits and drawbacks of simulators in comparison to conventional teaching methods.
MATERIALS AND METHODS: The results of using the Vimedix 3.2 virtual simulator in the teaching process were analyzed. Simulations of abdominal ultrasound, transthoracic echocardiography, and triplex scanning of major vessels were performed. The study included 26 residents specializing in ultrasound diagnosis and 37 physicians undergoing professional retraining courses.
RESULTS: Using a virtual simulator during the initial stage of training helps eliminate many of the challenges that residents and trainees encounter in clinical practice. The use of a simulator during testing appears to be less beneficial than during a practical examination employing ultrasound scanners and real patients.
CONCLUSION: The use of a simulator at the initial stage is advisable to get familiar with this research methodology. It is recommended to develop and use additional teaching materials and programs in training. The advantages of the virtual simulator include ease of use during the initial stages of training, a steep learning curve, and the availability of an extensive database of pathological cases. The identified noncritical shortcomings require correction during further training in the clinic.
Full Text
BACKGROUND
Virtual and simulation technologies have recently increased applications in various areas of medicine, including teaching medical students. Various simulations of real processes have long been used in the training and practice of specialists in numerous areas, and they have been developed for several decades [1–3]. This process is accelerating because of both the widespread digitization of our lives and the active implementation of such technology in clinical practice.
Virtual simulators and augmented reality technologies are increasingly being used in clinical practice, not only for diagnosis but also for therapeutic purposes in areas such as surgery, anesthesia, and resuscitation. These include three-dimensional (3D) anatomy and imaging tables, virtual reality programs for studying human anatomy, and surgical simulators and robots [4–6]. Consequently, digital methods are being used in teaching and knowledge assessment of medical graduates and healthcare professionals undergoing retraining during state certifications and accreditations, including ultrasound diagnostic specialists [1, 7]. The interest in such technologies increased because medical schools and postgraduate education institutions are finding it increasingly difficult to teach some specialties in clinical settings.
These include limitations specific to working in the clinic, such as research place and time constraints [7, 8], shortage of ultrasound machines, lack of mentors, and access issues during quarantine. Other challenges are related to the individuals being examined, including psychological pressure on students during their first interactions with patients, some patients’ reluctance to be examined by students [8], lack of patients with the pathology of interest in the clinic, and poor visualization in the so-called “difficult” patients. Moreover, some problems are related to students’ theoretical knowledge and level of engagement, which can significantly increase the time for practicing the required skills, which is limited in the clinic. Furthermore, skill building in ultrasound scanning techniques can be challenging because of a lack of understanding of normal and abnormal anatomy. This refers to the proper sensor placement, which can be time-consuming and uncomfortable for the patient.
Thus, changes in the teaching methods and curricula for some specialties in medical schools and the use of modern virtual and simulation devices are necessary. It is especially relevant in training radiology specialists because digital image processing software has long been used in X-ray diagnosis, and specialists must have adequate skills and expertise.
However, the experience of using such technologies in teaching medical students is limited. Consequently, original articles on the subject in both Russian and foreign literature are limited. The majority of these articles emphasize the benefits of simulation technologies in training ultrasound diagnostic specialists [7–10]; however, certain disadvantages exist, particularly in testing and knowledge assessment [7]. Virtually no standardized approaches have been established for simulation training in diagnostic ultrasonography, efficient use of virtual simulators, establishing their role in the educational process and evaluating the results of their use. Data on the development and effectiveness of special training modules and teaching materials aimed at mastering specific types of simulators are limited.
In this regard, we analyzed our experience with modern digital technologies in teaching and knowledge assessment, using an ultrasound simulator as an example. The virtual simulator has been used for 4 years for training of ultrasound diagnostic specialists at the Department of X-ray Diagnostics and Radiation Therapy of the Institute of Medicine of the Petrozavodsk State University. The simulator is intended for first- and second-year residents and physicians during professional retraining. The simulator is used by residents during the final state certification and for primary accreditation of ultrasound diagnostic specialists.
AIM
To determine the possibilities and algorithms for the use of a virtual ultrasound simulator to train ultrasound diagnostic specialists based on the results of using a simulator to assess the benefits and drawbacks of simulators in comparison with conventional teaching methods.
MATERIALS AND METHODS
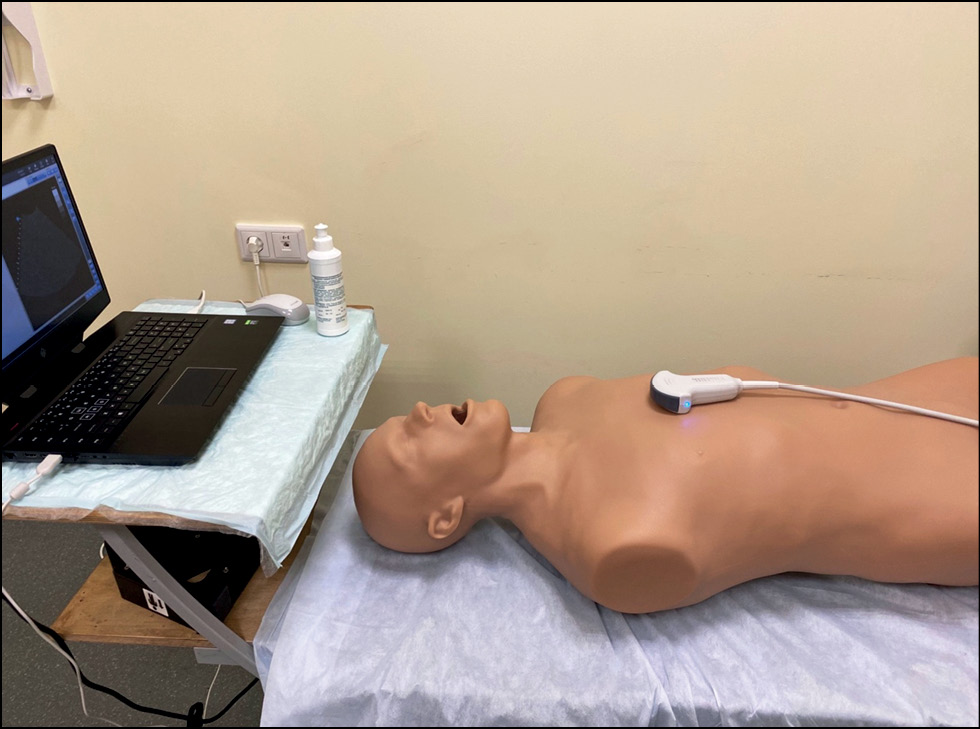
The results of using a Vimedix 3.2 virtual ultrasound simulator (CAE Healthcare, Canada) in the teaching process were analyzed. This simulator is the most widely available in both the Russian and foreign markets. It includes several mannequins and sensors for practicing ultrasound scanning techniques in various areas and an abnormal case database. The simulator includes an Omen laptop (Hewlett-Packard, USA) with wireless connection, a mouse, a male multipurpose mannequin, an array of ultrasonic convex sensor, and a sensor adapter (Fig. 1).

Fig. 1. Vimedix 3.2 virtual ultrasound simulator.
The laptop used comes with original ultrasound simulation software that supports both 2D and 3D/4D anatomical modes with multiplanar reconstruction. Microsoft HoloLens 2 (USA) mixed reality technology allows the user to visualize the anatomical structures of interest in the “live” mode, i.e., in motion. It is used to facilitate navigation in the area of interest by assessing X-ray tomographic images [11, 12] and in the simulator for correct sensor positioning during simulation [13]. In the laptop screen’s workspace, in addition to the 2D image, a separate window displays a 3D/4D animated anatomical image of the organs within the scanning area. Users can control the display of anatomical structures and split the window for better visualization.

Fig. 2. Simulation program interface in mixed reality and 2D modes.
The simulator can imitate procedures such as transabdominal ultrasonography, transthoracic echocardiography, and scanning of major vessels. The following scanning modes are available:
- В (2D, B-scan ultrasonography)
- М (A-scan ultrasonography)
- Color Doppler (CD)
- Pulsed wave (PW)
A customized marker system monitors the sensor movement along the mannequin surface, allowing for ultrasound scanning in various positions (dorsal, lateral, etc.). A set of basic tools was used to assess the results, such as length, area, volume, and blood flow velocity measurement in Doppler modes, and calculation of central hemodynamics parameters during echocardiography. A final protocol can be generated based on the scan findings and measurements.
The virtual simulator has a large database of ultrasound images depicting various pathologies of the abdominal organs and cardiovascular system. This allows the user to master ultrasound scanning techniques in various areas, both with normal anatomy and various pathologies. Consequently, during knowledge assessment, the ability of certification candidates to detect and describe various pathological changes using standard protocols can be evaluated.
The study included 26 residents training in diagnostic ultrasonography and 37 physicians undergoing professional retraining in the same discipline. Because the study used categorical data and two answer options, this sample size was sufficient to assess the proposed teaching method and extrapolate the results to all students training in ultrasonography, during the study period and beyond. The results of using the simulator were assessed by personnel of the Department of X-ray Diagnostics and Radiation Therapy and practicing diagnosticians from the institute’s clinical sites who participated in the training and knowledge assessment.
The main parameters for assessing the results of using the virtual simulator were those necessary for organizing and planning the teaching process:
- Time required to master the simulator (including training in running the software and using the interface)
- Ease of learning and psychological comfort
- Ease of handling the sensor and mannequin
- Correct sensor positioning (using anatomic landmarks of the mannequin and the mixed reality technology)
- Ability of students to use the simulator without assistance
- Need for special teaching materials and modifications of the existing training program.
Residents and students who had previously used ultrasound scanners in the clinic assessed the quality of images created by the simulator and compared it with the quality of the image obtained in a real world setting. Data were collected by an anonymous survey of students using the Likert scale [14] and scoring from 0 to 5 for the proposed questions (Figs. 3 and 4).

Fig. 3. Questionnaire for residents and students, part 1.

Fig. 4. Questionnaire for residents and students, part 2.
During training, the teacher analyzed the work with the equipment using the assessment criteria. At the end of the training course, teachers and mentors working in the clinic used tests to assess the theoretical knowledge and practical skills of the students. The majority of the assessment criteria were subjective, making it difficult to interpret the results. However, this is inherent in ultrasonography, contributing to its high operator dependency. Problems that emerged during training were also recorded, and their causes and solutions were discussed with the students.
Ethical considerations
The study volunteers participating in training and research provide informed consent. Data were acquired using a voluntary anonymous questionnaire survey, and no personal data were collected or processed during the process. This study did not involve any patients.
RESULTS
When assessing the benefits and drawbacks of using a virtual simulator in the training, the simulator was compared with the conventional method, where residents and physicians receive training using an ultrasound scanner in real patients in clinical settings under the supervision of mentors (department staff and practicing physicians). This conventional approach has well-known limitations, particularly in recent years because of the COVID-19 pandemic [15].
All residents and the majority of the students (81%) successfully completed the training with the virtual ultrasound simulator. The success criteria included confident use of the simulator software and interface (running, settings, etc.) and full mastery of ultrasound scanning techniques in various areas (Table 1).
Table 1. Student survey and testing results
Residents | Physicians | |
Number of students | 26 | 37 |
Successful mastery of the simulator | 100% | 81% |
Minimum time required to master the simulator, min | 90 | 135 |
Psychological comfort during training in diagnostic ultrasonography using the simulator | 80% | 68% |
Psychological comfort during preparation for testing/accreditation using the simulator | 90% | 75% |
Satisfactory quality of simulator images in the M and B modes | 95% | 95% |
Satisfactory quality of simulator images in Doppler modes | 90% | 89% |
Positive opinion on the use of 3D/4D navigation software | 100% | 100% |
Preference for the simulator during final testing and accreditation | 100% | 90% |
The minimum time required to master the simulator was 2–6 training sessions (2 academic hours each) under the supervision of a department teacher, plus one introductory lecture (1 academic hour, or 45 min). Notably, residents mastered the simulator more quickly than students. This, we believe, is due to their theoretical background (lectures in X-ray diagnosis) and experience in working with ultrasound equipment. For most residents (75%), 2–3 training sessions with a mentor were sufficient, after which they could work without supervision. As for physicians taking professional retraining, older students (aged ≥ 50 years) required a minimum of 3–4 and a maximum of 6 training sessions to master basic skills in using the simulator. Here, problems were encountered because some students (26%) had either zero or rudimentary computer skills. Consequently, they could not independently run laptop software and confidently use the simulator application interface even after completing the training course. To assess the results of using the virtual simulator, task-based tests were performed during the initial accreditation of ultrasound diagnostic specialists (Fig. 5).

Fig. 5. Tests to assess the results of mastering ultrasound scanning techniques.
When using the simulator to master basic skills in diagnostic ultrasonography, 72% of the students reported more psychological comfort than when training on real patients in clinical settings. This criterion was evaluated only by students who had some actual experience with ultrasound scanners (however limited). Both mentors and students stated that the simulator makes it easier and faster to master ultrasound scanning techniques. However, the stress of the first contact with a patient in a real world setting must be addressed in subsequent practice. This was primarily relevant for residents who had no experience with ultrasound scanning in real patients.
Working on the simulator was effortlessly integrated into the training program because it was placed on the premises of the medical school; thus, we did not have to adjust to the working hours of a healthcare facility. This helps us address the issue of a lack of space and limited time for training in clinical settings. We practiced dividing the students into groups, which allowed us to propose a training schedule convenient for the teacher and students. Accordingly, small groups of up to three students are most suited for simultaneous work on a virtual simulator. This group size is determined by the amount of time taken by one student to master new skills during a training session, as well as the size of the classroom.
Most students rated the image quality in the B and M modes as good (95%) and in the Doppler modes as satisfactory (89%). The assessment criteria included the difficulty in recognizing and interpreting the resulting images and the ability to correlate them with actual anatomical objects. A problem in using Doppler modes was the inability to adjust some of their parameters. Consequently, blood flow in CD and PW modes was only clearly visualized through the heart valves and some portions of the aorta.
All students agreed that an additional window with a mixed reality mode and 3D/4D-live anatomical navigation of the examined area helps in positioning the sensor when examining all areas. It was especially convenient when examining the abdominal organs and the heart [12].
In the B mode, an issue with incorrect sensor positioning on the mannequin for some standard projections of the heart (such as apical) was discovered, which will require improvement in the future when practicing on real patients. In these cases, students successfully solved the challenge using the mixed reality system, allowing them to assess accurately the section planes of the organ and the position of the sensor relative to anatomical landmarks.
According to the survey results, 95% (both residents and physicians) favored using the simulator over training on real patients. The mean time spent practicing ultrasound scanning in one area using the simulator was 1–2 training sessions (2 academic hours each). The training included multiple-view scanning with various positions of the mannequin; moreover, the duration was not limited to one scan, which is unavoidable in clinical settings. When our students began using real ultrasound scanners, their skills in ultrasound scanning of various areas were satisfactory, requiring only a quick correction of sensor positioning and the ability to work with “difficult” patients and during specific respiratory phases.
In teaching methodology, it should differ from training in clinical settings under the supervision of mentors. Training in clinical settings includes two main approaches: witnessing the procedure and imitating the mentor’s actions on a patient. Training using a virtual simulator also offers an opportunity for self-learning through trial and error. This approach is more comfortable for students (at least because there are no time constraints or psychological pressures) and can provide better practical results. This training strategy enabled our students to work on the simulator independently and on their schedule. If necessary, the teacher provided consultations remotely via voice and video communications.
Furthermore, the conventional “one mentor, one trainee” approach could be converted to group training at the initial stage, which is more economically viable. The simulator allowed the merging of the theoretical and practical components of the training program in a single training session. Initially, the teacher presents an introductory lecture on a certain topic with a demonstration of the simulator. Then, the students could reinforce their knowledge during practical training (Fig. 6). This approach proved convenient when learning the fundamentals of ultrasound scanning in specific areas and when preparing for testing.

Fig. 6. A second-year resident using the simulator.
The use of the virtual simulator for knowledge assessment during resident certification and specialist accreditation yielded ambiguous results, requiring further discussion. In several similar studies, the authors emphasize the benefits of using simulators, particularly the lack of stress for certification candidates and conditions close to reality [8, 15]. These findings are consistent with the views of most students (95%), who chose to use the simulator during practical testing. Furthermore, this judgment was consistent before and after testing. However, according to the department staff and mentors, this testing option has more negatives than positives.
DISCUSSION
Based on the results obtained with the Vimedix 3.2 virtual simulator, it can be recommended for use at the initial stage of training ultrasound diagnostic specialists. Our experience confirmed the benefits of incorporating virtual and augmented reality technologies into educational programs for medical students and ultrasound training programs as reported previously [8–10, 15]. Virtual simulators are useful for practicing ultrasound scanning techniques in specific areas, positioning the sensor using anatomical landmarks, and learning how to take basic measurements in various modes, including Doppler ones. However, they do not replace clinical experience, but augment it. At subsequent stages, practical skills should be reviewed (and improved) by examining real patients under the supervision of a mentor.
Currently, little information exists on how skills gained through simulation-based training correlate with clinical efficacy or how long they will be maintained [16, 17]. Thus, practical testing is essential in graduates several years after the start of independent work to more accurately assess the efficacy of training. The Objective Structured Assessment of Ultrasound Skills scale can be used for this purpose [18].
To effectively master the simulator, a user manual that addresses topics such as running the application, a user manual for the interface, and step-by-step instructions for specific tasks is necessary. To facilitate self-learning, the teacher should prepare an introductory lecture to familiarize residents and students with the simulator software and demonstrate its capabilities. Accordingly, guidelines for examining specific anatomical areas of the mannequin using a simulator will also be beneficial. To master ultrasound scanning techniques in specific areas, training modules lasting two academic hours proved useful, with one to demonstrate the techniques and the other for practical training. Because of the varying computer skills of students, the training program can provide two options, with more or less time spent on training in running simulator software.
To fully master the simulator, a minimum of 5–6 training sessions with a teacher covering several scanning areas are required. These could include reviewing the normal anatomy, practicing positioning, various ultrasound modes, and organ assessment parameters. Students can then work independently on their schedule, including with remote supervision from the teacher to address any emerging concerns. Furthermore, using the pathological case database integrated into the software, the virtual simulator can be used for training in the diagnosis of disorders that were not encountered in real patients in clinical settings.
However, the final knowledge assessment should be performed on real patients using ultrasound scanners because this allows assessing the ability of certification candidates to handle specific clinical situations. An optimal, albeit more complex, approach is to perform ultrasound scans in both healthy individuals and patients with a specific condition, for the resident or student to demonstrate to the mentor and accurately describe a standard protocol. Residents and students prefer using a simulator because preparing for and performing the practical test on a simulator is psychologically more comfortable than in clinical settings. Using a simulator does not require much time, patient participation, or clinical equipment; it can be used independently at any time, and students are not stressed.
Conversely, teachers believe that preparing for practical tests is primarily about memorizing certain actions. During testing, experts mainly assess the execution and sequence of certain actions rather than their quality and results. The checklist and remote monitoring system do not allow for a detailed assessment of the accuracy of images obtained by certification candidates and the assignment of additional tasks in the case of doubt. Work with various body types could not be assessed; standardized normal anatomical images in the absence of respiratory movements are assessed, and multiple-view scanning is not performed. The emphasis is more on the existing testing methods and principles rather than the operating principles and capabilities of virtual simulators.
The hardware and software features of the Vimedix 3.2 virtual simulator allow for the appropriate simulation of the primary scanning techniques that an ultrasound specialist should master during training. Accordingly, this simulator can be further improved, and its scope broadened to include training in modern techniques such as ultrasound-guided punctures of various organs and gastrointestinal echoendoscopy.
CONCLUSION
The Vimedix 3.2 simulator is recommended for use at the initial training stage for ultrasound diagnostic specialists to practice ultrasound scanning techniques in various areas, including specific clinical situations. In our opinion, using the simulator for certification and accreditation is currently less preferable than testing on real patients in clinical settings. To use the simulator effectively, additional teaching materials and training modules and reviewing the practical training approaches must be implemented.
The main benefits of using the Vimedix 3.2 virtual simulator for educational purposes are psychological comfort for students, a steep learning curve, possibility to work in a group, an extensive pathological case database, and placement on the premises of the medical school.
The identified drawbacks include the inability to practice skills required to work with real patients, errors in sensor positioning, and inconsistent image quality in the CD mode. These drawbacks are not critical, but they necessitate subsequent adjustments to the acquired skills when working in the clinic.
ADDITIONAL INFORMATION
Funding source. This study was not supported by any external sources of funding.
Competing interests. The authors declare that they have no competing interests.
Authors’ contribution. All authors made a substantial contribution to the conception of the work, acquisition, analysis, interpretation of data for the work, drafting and revising the work, final approval of the version to be published and agree to be accountable for all aspects of the work. V.A. Vasiliev — concept and design of the study, data analysis, writing the text of the article; S.N. Kondrichina — collection and processing of materials.
About the authors
Valeri А. Vasilev
Petrozavodsk State University
Email: valerij-vasiljev@list.ru
ORCID iD: 0000-0001-7164-4274
SPIN-code: 3582-0940
MD, Cand. Sci. (Medicine), Assistant Professor
Russian Federation, PetrozavodskSvetlana N. Kondrichina
Petrozavodsk State University
Author for correspondence.
Email: konsvet12@gmail.com
ORCID iD: 0000-0001-8472-9146
MD, Cand. Sci. (Medicine), Assistant Professor
Russian Federation, PetrozavodskReferences
- Meller G. A typology of simulators for medical education. J Digit Imaging. 1997;10(Suppl. 1):194–196. doi: 10.1007/BF03168699
- Gaba DM. The future vision of simulation in health care. Quality and Safety in Health Care. 2004;13(Suppl. 1):2–10. doi: 10.1136/qshc.2004.009878
- Alinier G. A typology of educationally focused medical simulation tools. Medical Teacher. 2007;29(8):243–250. doi: 10.1080/01421590701551185
- Gorshkov MD, Nikitenko AI. Review of russian and world experience: usage of virtual simulators in training of endosurgeons. Virtual’nye tekhnologii v meditsine. 2009;1(1):15–18. EDN: QBAVGC doi: 10.46594/2687-0037_2009_1_18
- Gorshkov MD, Fedorov AV. Classification of the simulation equipment. Virtual’nye tekhnologii v meditsine. 2012;2(8):23–35. EDN: BJWHJB doi: 10.46594/2687-0037_2012_2_21
- Svistunov AA, editor. Simulation training in medicine. Moscow: Sechenov University Publishing; 2013. (In Russ). EDN: XVVEDZ doi: 10.46594/9785423501099
- Chalouhi GE, Bernardi V, Gueneuc A, et al. Evaluation of trainees’ ability to perform obstetrical ultrasound using simulation: challenges and opportunities. Am J Obstet Gynecol. 2016;214(4):525–528. doi: 10.1016/j.ajog.2015.10.932
- Hani S, Chalouhi G, Lakissian Z, Sharara-Chami R. Introduction of Ultrasound Simulation in Medical Education: Exploratory Study. JMIR Med Educ. 2019;5(2):13568. doi: 10.2196/13568
- Ovsiannikova LS, Shunkova SA, Kespleri EV. The importance of simulation technologies in improving the quality of training of specialists in ultrasound diagnostics. VI International (76 All-Russian) Scientific and Practical Conference “Topical Issues of Modern Medical Science and Public Health”. 2021;3:642–645.
- Freundt P, Nourkami-Tutdibi N, Tutdibi E, et al. Controlled Prospective Study on the Use of Systematic Simulator-Based Training with a Virtual, Moving Fetus for Learning Second-Trimester Scan: FESIM III. Ultraschall Med. 2023;44(4):e199–e205. doi: 10.1055/a-1984-8320
- Hatzl J, Böckler D, Hartmann N, et al. Mixed reality for the assessment of aortoiliac anatomy in patients with abdominal aortic aneurysm prior to open and endovascular repair: Feasibility and interobserver agreement. Vascular. 2023;31(4):644–653. doi: 10.1177/17085381221081324
- Kukla P, Maciejewska K, Strojna I, et al. Extended Reality in Diagnostic Imaging-A Literature Review. Tomography. 2023;9(3):1071–1082. doi: 10.3390/tomography9030088
- Vasilev VA, Vasileva AE. 3D/4D anatomical navigation in virtual ultrasound simulators. Actual issues of fundamental and clinical morphology: Proceedings of the International Scientific and Practical Conference, Tver, October 14, 2022. 2022:101–105. EDN: TWYHTL
- Bernstein IH. Likert Scale Analysis. Elsevier; 2005. doi: 10.1016/B0-12-369398-5/00104-3
- Dietrich CF, Lucius C, Nielsen MB, et al. The ultrasound use of simulators, current view, and perspectives: Requirements and technical aspects (WFUMB state of the art paper). Endosc Ultrasound. 2023;12(1):38–49. doi: 10.4103/EUS-D-22-00197
- Almestehi M, Alomaim W, Rainford L, et al. Role of the virtual reality simulator (ScanTrainer) as a multidisciplinary training tool in transvaginal ultrasound: A systematic review and narrative synthesis. Radiography (Lond). 2019;25(3):260–268. doi: 10.1016/j.radi.2018.12.009
- Pezel T, Dreyfus J, Mouhat B, et al. Effectiveness of Simulation-Based Training on Transesophageal Echocardiography Learning: The SIMULATOR Randomized Clinical Trial. JAMA Cardiol. 2023;8(3):248–256. doi: 10.1001/jamacardio.2022.5016
- Tolsgaard MG, Todsen T, Sorensen JL, et al. International multispecialty consensus on how to evaluate ultrasound competence: a Delphi consensus surve. PLoS One. 2013;8(2):e57687. doi: 10.1371/journal.pone.0057687
Supplementary files

