

")








Radiographic markers of cardiovascular risk based on digital mammograms: a cross-sectional study
- Authors: Tsurskaya D.D.1, Mershina E.A.1, Sinitsyn V.E.1, Ivlev O.E.1, Filichkina E.M.1, Yarovaya E.B.1, Dolgushin G.O.1, Orlova I.А.1
-
Affiliations:
- Lomonosov Moscow State University
- Issue: Vol 6, No 3 (2025)
- Pages: 398-413
- Section: Original Study Articles
- Submitted: 27.12.2024
- Accepted: 21.07.2025
- Published: 12.09.2025
- URL: https://jdigitaldiagnostics.com/DD/article/view/643487
- DOI: https://doi.org/10.17816/DD643487
- EDN: https://elibrary.ru/VQGCFY
- ID: 643487

Cite item
Full Text

Abstract
BACKGROUND: Studies have demonstrated an association between cardiovascular risk and mammographic density and breast arterial calcification. However, their combined impact remains poorly understood.
AIM: This study aimed to evaluate the correlation between mammographic density, breast artery calcification, and cardiovascular risk category in asymptomatic women aged ≥40 years.
METHODS: This retrospective, single-center, selective study included women who underwent preventive screening mammography at the University Clinic of Lomonosov Moscow State University between 2019 and 2023. The Systematic Coronary Risk Evaluation 2 was used to determine cardiovascular risk categories. A radiologist evaluated mammograms at a workstation to obtain data on mammographic density and glandular calcifications. The data were analyzed using a machine learning technique called Uniform Manifold Approximation and Projection. Univariate logistic regression was employed to calculate odds ratios and 95% confidence intervals. The reference group included mammograms showing high breast density and no calcifications. The odds ratio for each selected group is presented relative to the reference. The contingency tables were assessed using Pearson’s chi-squared (χ2) test. The significance level for all tested hypotheses was set at 0.05.
RESULTS: The mammograms of 1030 women aged 40–89 years were evaluated. Based on the study results, eight groups (G7–G0) were formed, depending on combinations of the following criteria: high or low glandular density, presence or absence of vascular and nonvascular calcification, and extent of calcification. Women with low mammographic density and vascular calcifications in more than one quadrant were found to have a >75% likelihood of high or extremely high cardiovascular risk. The probability exceeded 90% for a combination of vascular and nonvascular calcifications in two or more quadrants.
CONCLUSION: A correlation was found between calcifications, mammographic density, and cardiovascular risk category.
Full Text
ОБОСНОВАНИЕ
Согласно данным исследований и клинических рекомендаций, маммография является основным методом скрининга рака молочной железы и рекомендована женщинам начиная с 40 лет — ежегодно или один раз в два года [1, 2].
Этот метод лучевой диагностики продемонстрировал высокую эффективность в раннем выявлении злокачественных новообразований, зарекомендовав себя как быстрый, доступный и экономически обоснованный метод диагностики, позволяющий охватывать широкие группы женского населения [1, 2].
В связи с этим особый интерес представляет возможность использования маммографии не только для диагностики рака молочной железы, но и для получения дополнительной информации о состоянии здоровья женщин. В частности, выявление на маммограммах признаков, ассоциированных с повышенным риском социально значимых заболеваний, таких как ишемическая болезнь сердца и атеросклероз, открывает перспективы для расширения профилактических мероприятий и может способствовать улучшению прогноза пациенток [3, 4].
Установлено, что кальциноз стенок маммарных артерий обладает высокой информативность в отношении риска кальцификации коронарных артерий, которую рассматривают как достоверный маркёр коронарного атеросклероза и ишемической болезни сердца, а также значимый предиктор неблагоприятных сердечно-сосудистых событий [3–5]. Морфологически кальциноз медии артерий молочной железы отличается от интимального атеросклеротического поражения стенок коронарных артерий, связанного с ишемической болезнью сердца. Тем не менее проведённые исследования подтверждают наличие статистически значимой корреляции между кальцификацией стенок артерий молочной железы и сердечно-сосудистыми факторами риска, а также распространённостью ишемической болезни сердца [6].
По данным последних исследований стало очевидно, что маммографическим маркёром риска сердечнососудистых событий могут выступать не только сосудистые кальцинаты. Так, в литературном обзоре Е.В. Бочкарёвой и соавт. [7], основанном на анализе данных крупных когортных исследований, продемонстрировано, что рентгенологическая плотность молочной железы также является предиктором развития неблагоприятных сердечно-сосудистых событий. C. Sardu и соавт. [8] установили, что у женщин, имевших до наступления менопаузы наименьшую рентгенологическую плотность молочной железы [тип ACR (American College of Radiology) А], 10-летняя частота крупных неблагоприятных сердечно-сосудистых событий составила 19,6%, что в несколько раз превышало аналогичный показатель у женщин с более высокой рентгенологической плотностью молочной железы: 7,6, 3,3 и 2% для категорий ACR B, C и D соответственно. Кроме того, наличие низкой рентгенологической плотности молочной железы (ACR А) в пременопаузе ассоциировано с троекратным увеличением 10-летнего риска развития сердечно-сосудистых событий. Несмотря на возрастающий интерес к изучению взаимосвязи маммографических признаков и риска сердечно-сосудистых заболеваний (ССЗ), существующие работы в данной области имеют определённые ограничения, что затрудняет широкое применение полученных данных в клинической практике.
- Во-первых, в литературе сохраняется неоднозначность в отношении диагностической и прогностической ценности кальцинатов молочных артерий как маркёра сердечно-сосудистого риска. Данный показатель не включён в международные рекомендации по диагностике и профилактике ССЗ, что ограничивает его признание в клинических алгоритмах [4].
- Во-вторых, методологические ограничения ранее проведённых исследований также существенно снижают возможность обобщения их результатов. Некоторые работы выполнены с использованием одномоментного дизайна исследования без длительного последующего наблюдения [5, 6], что исключает возможность оценить динамику развития ССЗ и их осложнений. Кроме того, кальциноз молочных артерий зачастую оценивают с использованием упрощённой бинарной классификации («присутствует» или «отсутствует»), без количественной характеристики степени кальцификации [5, 6], что снижает чувствительность оценки.
Особый интерес представляют исследования, в которых кальцинаты молочных артерий рассматривают не изолировано, а в сочетании с другими маммографическими маркёрами. Так, E. Aldous и соавт. [9] установили, что комплексная оценка рентгенологической плотности молочной железы и кальцификации молочных артерий повышает прогностическую точность в отношении риска развития ишемической болезни сердца по сравнению с анализом каждого из этих показателей по отдельности.
Это указывает на перспективность комплексного подхода, а также подчёркивает необходимость разработки и внедрения стандартизированных протоколов оценки. Вместе с тем большинство предыдущих исследований не учитывало совокупное влияние рентгенологической плотности молочных желёз и наличия кальцинатов в молочных артериях на риск ССЗ [6–8]. Тем не менее данные маркёры отражают различные аспекты сосудистого и гормонального статуса женщины и потенциально могут обладать синергетическим прогностическим значением.
ЦЕЛЬ
Оценка взаимосвязи рентгенологической плотности молочной железы и выраженности кальциноза в стенках её артерий с категорией риска сердечно-сосудистых заболеваний у асимптомных женщин 40 лет и старше.
МЕТОДЫ
Дизайн исследования
Проведено одномоментное одноцентровое выборочное исследование.
Условия проведения
В исследование включали данные женщин, проходивших профилактическое маммографическое обследование в Университетской клинике Московского государственного университета имени М.В. Ломоносова в период с 2019 по 2023 год. Смещения запланированных временных интервалов не было.
Продолжительность исследования
Исследование проведено в период с сентября по декабрь 2024 года.
Критерии соответствия
Критерии включения:
- женщины с результатами профилактической рентгеновской маммографии;
- женщины в возрасте 40 лет и старше;
- проведение профилактической рентгеновской маммографии на базе Университетской клиники Московского государственного университета имени М.В. Ломоносова в период с 2019 по 2023 год.
Критерии невключения:
- наличие артефактов на маммограмме;
- выполнение профилактической маммографии с ошибками (нестандартная укладка, неполный охват железы).
Критерии исключения:
- отсутствие в медицинских картах данных, необходимых для расчёта сердечно-сосудистого риска;
- установленный диагноз ишемической болезни сердца.
Профилактическая маммография
Рентгеновскую маммографию проводили с использованием цифрового аппарата General Electric Senographe Essential® (GE Healthcare, США) в двух проекциях.
Для получения данных о рентгенологической плотности молочных желёз и видах кальцинатов в каждой молочной железе, врач-рентгенолог анализировал снимки, выполненные в краниокаудальной и медиолатеральной проекциях, на рабочей станции SenoIris® (GE Healthcare, США).
Целевые показатели исследования
Основной показатель исследования
В качестве основного показателя исследования рассматривали взаимосвязь рентгенологической плотности молочной железы и наличия кальциноза её артерий с категорией риска ССЗ.
Методы измерения целевых показателей
Оценка плотности молочных желёз
Для интерпретации результатов маммографии использовали систему международной шкалы BI-RADS (Breast Imaging Reporting and Data System) [10].
Плотность молочных желёз оценивали с использованием общепринятой шкалы, предложенной Американской коллегией радиологов (American College of Radiology) и входящей в стандарты описания шкалы BI-RADS [10]. В соответствии с данной шкалой выделяют четыре типа плотности молочной железы (рис. 1).

Рис. 1. Шкала плотности молочных желёз Американской коллегии радиологов: a — ACR A; b — ACR B; c — ACR C; d — ACR D. ACR (American College of Radiology) — Американская коллегия радиологов.
Для удобства представления данных ACR в таблицах общепринятые буквенные обозначения типов плотности мы заменили на числовые:
- А(1) — ткань железы имеет преимущественно жировую плотность (плотность — здесь идалее характеризует степень ослабления рентгеновского излучения приего прохождении черезткань железы). Маммография обладает высокой чувствительностью вдиаг-ностике патологических очагов;
- В(2) — отмечены отдельные участки фибро-гландулярной (фиброзно-железистой) низкой рентгенологической плотности;
- С(3) — железа неоднородной (гетерогенной) высокой плотности либо отдельные участки молочных желёз достаточно плотные имогут скрывать небольшие образования;
- D (4) — очень плотные железы. Маммография обладает низкой чувствительностью в диагностике патологических очагов.
Оценка кальциноза стенок артерий молочных желёз
Тип кальциноза стенок артерий молочных желёз оценивали с использованием следующей шкалы, которую мы разработали:
- 1 — отсутствие кальцинатов;
- 2 — только несосудистые кальцинаты;
- 3 — только сосудистые кальцинаты;
- 4 — сосудистые и несосудистые кальцинаты.
Кроме того, учитывали распространённость вовлечённых квадрантов молочной железы по следующей шкале:
- 0 — отсутствие вовлечённых квадрантов;
- 1 — один квадрант;
- 2 — два;
- 3 — три и четыре.
В свою очередь, количество кальцинатов в квадранте учитывали в соответствии со следующей шкалой:
- 0 — отсутствие кальцинатов;
- 1 — единичные;
- 2 — множественные.
Оценка категории риска сердечно-сосудистых заболеваний
Категорию риска ССЗ определяли в соответствие с рекомендациями Российского кардиологического общества с использованием шкалы SCORE2 (Systematic Coronary Risk Estimation 2) [11].
Данные, необходимые для оценки 10-летнего риска фатальных и нефатальных ССЗ, получали из медицинских карт пациенток. При этом учитывали следующие модифицируемые и немодифицируемые факторы:
- возраст;
- индекс массы тела;
- наличие вредных привычек (курение);
- концентрация глюкозы;
- концентрация общего холестерина;
- систолическое артериальное давление;
- отягощённый анамнез: наличие сахарного диабета 2-го типа, артериальной гипертензии, ССЗ.
Анализ в группах
Сформировано 10 различных подгрупп пациенток (G0–G9) в зависимости от наличия кальцинатов, плотности молочных желёз, типа кальцинатов и числа вовлечённых квадрантов (1 или 2 и более) (табл. 1).
Таблица 1. Критерии первоначально сформированных групп | ||
Группа | Шифр | Описание |
G9 | {1,2} (3,23,*) |
|
G8 | {1,2} (2,23,*) |
|
G7 | {1,2} (23,1,*) |
|
G6 | {1,2} (1,123,*) |
|
G5 | {1,2} (0,0,0) |
|
G4 | {3,4} (3,23,*) |
|
G3 | {3,4} (2,23,*) |
|
G2 | {3,4} (23,1,*) |
|
G1 | {3,4} (1,123,*) |
|
G0 | {3,4} (0,0,0) |
|
Кроме того, применяли современный метод машинного обучения UMAP (Uniform Manifold Approximation & Projection). Данный алгоритм разработали L. McInnes и соавт. [12] в 2020 году. Он является одним из самых современных среди всего семейства методов снижения размерности. Отличительная особенность данного метода — достаточно высокая скорость работы по сравнению с другими алгоритмами. Задача метода UMAP — моделирование многообразия с нечёткой топологической структурой (Fuzzy Topological Structure) на основе заданного набора данных (точек) и последующее его вложение в низкоразмерную проекцию данных, которая имеет максимально близкую нечёткую эквивалентную топологическую структуру. По результатам его применения на данных рентгеновской маммографии пациентки разделены на три кластера:
- I кластер — высокая плотность железы (ACR С или D) без кальцинатов;
- II кластер — низкая плотность железы (ACR A или B) без кальцинатов;
- III кластер — наличие любых кальцинатов вне зависимости от плотности железы.
Далее мы провели более детальный анализ в III кластере (пациентки с наличием кальцинатов), в результате которого сформировали итоговые 8 групп (G7–G0) (табл. 2).
Таблица 2. Критерии восьми итоговых групп | ||
Группа | Шифр | Описание |
G7 | {1,2} (3,23,*) |
|
G6 | {1,2} (2,23,*) |
|
G5 | {1,2} (23,1,*) |
|
G4 | {1,2} (1,123,*) |
|
G3 | {1,2} (0,0,0) |
|
G2 | {3,4} (123,23,*) |
|
G1 | {3,4} (123,1,*) |
|
G0 | {3,4} (0,0,0) |
|
Разделение по типу кальцинатов и числу вовлечённых квадрантов железы основано на бинарной логистической регрессии, где зависимой переменной стала категория риска ССЗ, принимающая два значения: 0 (низкий и умеренный риск) и 1 (высокий и очень высокий риск).
Группы сравнивали по категории риска ССЗ, используя отношения шансов (ОШ). За референсное значение принимали самую «благоприятную» группу по данным маммографии — группа с высокой плотностью молочных желёз (ACR С или D) и без кальцинатов. ОШ для выделенных групп приведено по отношению к референсу.
Этическая экспертиза
Протокол исследования одобрен локальным этическим комитетом Медицинского научно-образовательного центра Московского государственного университета имени М.В. Ломоносова (протокол № 5 от 16.10.2023). Перед проведением рентгеновской маммографии пациентки подписывали согласие на проведение исследования. Обработка материала проводилась ретроспективно, дополнительное согласие пациентки не подписывали.
Статистический анализ
В связи с тем, что заранее определён период последовательного включения пациенток в выборку, её размер предварительно не рассчитывали.
Статистический анализ проведён в среде R 4.4.2 с открытым исходным кодом. Возраст представлен в виде M±SD, где M — среднее значение, а SD — стандартное отклонение. Качественные показатели описаны абсолютными значениями и их долями (%). Кластеризацию проводили с помощью метода машинного обучения UMAP. ОШ и 95% доверительный интервал (ДИ) для них построены с помощью однофакторной логистической регрессии. Для анализа таблиц сопряжённости использовали критерий χ2 Пирсона. Для формирования групп по тяжести поражения на основе данных маммографии применяли многофакторную логистическую регрессию. Уровень значимости для всех проверяемых гипотез p=0,05.
РЕЗУЛЬТАТЫ
Характеристики выборки
Выборка состояла из 1030 женщин в возрасте от 40 до 89 лет, прошедших профилактическую маммографию на базе Университетской клиники Московского государственного университета имени М.В. Ломоносова. Распределение пациенток в зависимости от категории риска ССЗ в соответствии со шкалой SCORE2 продемонстрировано в табл. 3. Следует отметить, что наибольшее количество женщин характеризовались умеренным риском развития ССЗ — 33,7%.
Таблица 3. Распределение пациенток в зависимости от категории риска сердечно-сосудистых заболеваний на основе оценки SCORE2 | |
Категория риска | n (%) |
Низкий риск | 36 (3,5) |
Умеренный риск | 347 (33,7) |
Высокий риск | 306 (29,7) |
Очень высокий риск | 341 (33,1) |
Примечание. SCORE2 (Systematic Coronary Risk Estimation 2) — шкала для оценки 10-летнего риска развития сердечно-сосудистых заболеваний. | |
В табл. 4 представлена характеристика 10 первоначально сформированных групп пациенток (G9–G0) в зависимости от рентгенологической плотности молочных желёз, наличия и типа кальцинатов, а также числа вовлечённых квадрантов (1 или 2 и более). Результаты рентгеновской маммографии в зависимости от группы G9–G0 продемонстрированы на рис. 2–11 соответственно.
Таблица 4. Характеристика десяти первоначально сформированных групп для левой и правой молочной железы | |||||
Группа | Молочная железа | n (%) | Средний возраст, лет | Высокий и очень высокий риск ССЗ, n (%) | Отношение шансов (95% доверительный интервал) |
G9 | Левая | 100 (9,7) | 70,3±7,6 | 92 (92) | 23,7 (9,9–63,8) |
Правая | 95 (9,2) | 70,1±7,6 | 86 (90,5) | 19 (8,3–48,4) | |
G8 | Левая | 179 (17,4) | 63,7±8,9 | 135 (75,4) | 6,4 (3,6–11,6) |
Правая | 175 (17) | 63,5±9,2 | 132 (75,4) | 6,2 (3,5–11) | |
G7 | Левая | 190 (18,4) | 63,1±9,4 | 131 (68,9) | 4,6 (2,7–8,2) |
Правая | 205 (19,9) | 63±9,5 | 142 (69,3) | 4,5 (2,7–7,9) | |
G6 | Левая | 49 (4,8) | 65,5±8,7 | 33 (67,3) | 4,3 (2–9,7) |
Правая | 52 (5) | 66,3±8,4 | 38 (73,1) | 5,4 (2,5–12,4) | |
G5 | Левая | 222 (21,6) | 59,2±9,4 | 125 (56,3) | 2,7 (1,6–4,7) |
Правая | 213 (20,7) | 59,2±9,3 | 117 (54,9) | 2,5 (1,5–4,2) | |
G4 | Левая | 21 (2) | 69,8±9,9 | 16 (76,2) | 6,6 (2,1–25,3) |
Правая | 26 (2,5) | 69,4±10,7 | 21 (80,8) | 8,4 (2,8–30,9) | |
G3 | Левая | 78 (7,6) | 58,6±11,4 | 39 (50) | 2,1 (1,1–4,1) |
Правая | 68 (6,6) | 58,4±11,9 | 31 (45,6) | 1,7 (0,9–3,3) | |
G2 | Левая | 91 (8,8) | 57±10,7 | 40 (44) | 1,6 (0,9–3,1) |
Правая | 83 (8,1) | 56,5±10,4 | 40 (48,2) | 1,9 (1–3,6) | |
G1 | Левая | 6 (0,6) | 72,2±14,9 | 5 (83,3) | 10,3 (1,1–502,9) |
Правая | 9 (0,9) | 66,8±13,5 | 6 (66,7) | 4 (0,8–26,2) | |
G0 | Левая | 93 (9) | 53,1±10,4 | 30 (32,3) | Референс |
Правая | 103 (10) | 54,1±10,6 | 34 (33) | Референс | |
Примечание. ССЗ — сердечно-сосудистые заболевания. | |||||

Рис. 2. Группа G9: низкая плотность молочных желёз, сосудистые и несосудистые кальцинаты с вовлечением двух и более квадрантов.

Рис. 3. Группа G8: низкая плотность молочных желёз, только сосудистые кальцинаты с вовлечением двух и более квадрантов.

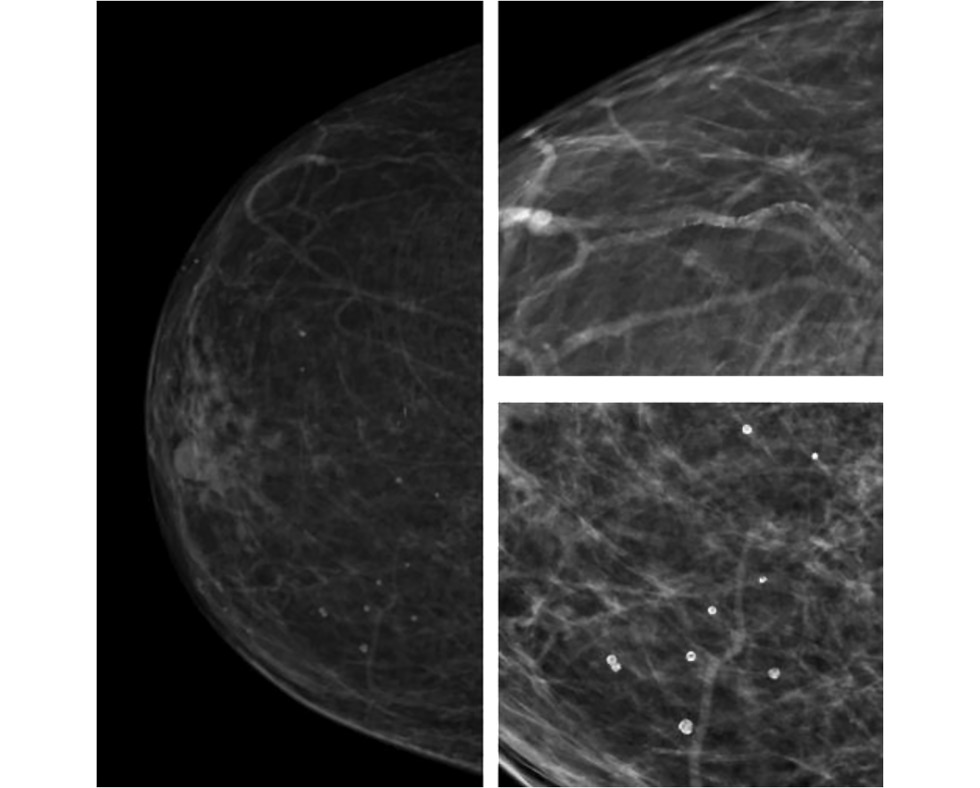
Рис. 4. Группа G7: низкая плотность молочных желёз, только сосудистые или сосудистые и несосудистые кальцинаты с вовлечением одного квадранта.

Рис. 5. Группа G6: низкая плотность молочных желёз, только несосудистые кальцинаты.

Рис. 6. Группа G5: низкая плотность молочных желёз, отсутствие кальцинатов.

Рис. 7. Группа G4: высокая плотность молочных желёз, сосудистые и несосудистые кальцинаты с вовлечением двух и более квадрантов.

Рис. 8. Группа G3: высокая плотность молочных желёз, только сосудистые кальцинаты с вовлечением двух и более квадрантов.

Рис. 9. Группа G2: высокая плотность молочных желёз, только сосудистые или их сочетание с несосудистыми кальцинатами с вовлечением одного квадранта.

Рис. 10. Группа G1: высокая плотность молочных желёз, только несосудистые кальцинаты.

Рис. 11. Группа G0: высокая плотность молочных желёз, отсутствие кальцинатов.
В результате применения метода машинного обучения UMAP к данным рентгеновской маммографии пациентки разделены на три кластера: I кластер (n=93); II кластер (n=222); III кластер (n=715). После детального анализа в III кластере (пациентки с наличием кальцинатов) сформированы итоговые 8 групп (G7–G0), характеристика которых продемонстрирована в табл. 5.
Таблица 5. Характеристики восьми итоговых сформированных групп для левой и правой молочных желёз | |||||
Группа | Молочная железа | n (%) | Средний возраст, лет | Высокий и очень высокий риск ССЗ, n (%) | Отношение шансов (95% доверительный интервал) |
G7 | Левая | 100 (9,7) | 70,3±7,6 | 92 (92) | 23,7 (9,9–63,8) |
Правая | 95 (9,2) | 70,1±7,6 | 86 (90,5) | 19 (8,3–48,4) | |
G6 | Левая | 179 (17,4) | 63,7±8,9 | 135 (75,4) | 6,4 (3,6–11,6) |
Правая | 175 (17) | 63,5±9,2 | 132 (75,4) | 6,2 (3,5–11) | |
G5 | Левая | 190 (18,4) | 63,1±9,4 | 131 (68,9) | 4,6 (2,7–8,2) |
Правая | 205 (19,9) | 63±9,5 | 142 (69,3) | 4,5 (2,7–7,9) | |
G4 | Левая | 49 (4,8) | 65,5±8,7 | 33 (67,3) | 4,3 (2–9,7) |
Правая | 52 (5) | 66,3±8,4 | 38 (73,1) | 5,4 (2,5–12,4) | |
G3 | Левая | 222 (21,6) | 59,2±9,4 | 125 (56,3) | 2,7 (1,6–4,7) |
Правая | 213 (20,7) | 59,2±9,3 | 117 (54,9) | 2,5 (1,5–4,2) | |
G2 | Левая | 103 (10) | 61,8±12,4 | 59 (57,3) | 2,8 (1,5–5,3) |
Правая | 98 (9,5) | 61,6±12,6 | 54 (55,1) | 2,5 (1,4–4,6) | |
G1 | Левая | 93 (9) | 57±10,6 | 41 (44,1) | 1,7 (0,9–3,1) |
Правая | 88 (8,5) | 57,2±10,9 | 44 (50) | 2 (1,1–3,8) | |
G0 | Левая | 93 (9) | 53,1±10,4 | 30 (32,3) | Референс |
Правая | 103 (10) | 54,1±10,6 | 34 (33) | Референс | |
Примечание. ССЗ — сердечно-сосудистые заболевания. | |||||
Основные результаты исследования
Высокая рентгенологическая плотность молочной железы при наличии кальцинатов ассоциирована с меньшей вероятностью высокой и очень высокой категории риска ССЗ в сравнении с низкой рентгенологической плотностью и наличием кальцинатов. Наибольшую ассоциацию с высокой и очень высокой категорией риска ССЗ демонстрировали группы G9 и G8. В свою очередь, отсутствие кальцинатов соответствует минимальной вероятности высокого и очень высокого риска ССЗ (см. табл. 4).
Установлена статистически значимая связь между числом вовлечённых квадрантов и выраженностью поражений как левой, так и правой молочной железы (табл. 6), p <0,001.
Таблица 6. Связь числа вовлечённых квадрантов с выраженностью кальциноза | ||||
Число вовлечённых квадрантов | Левая молочная железа, n (%) | Правая молочная железа, n (%) | ||
выраженность поражения | ||||
1 | 2 | 1 | 2 | |
1 | 278 (87 7) | 39 (12,3) | 294 (89,4) | 35 (10,6) |
2 | 99 (73,3) | 36 (26,7) | 83 (68) | 39 (32) |
3 | 97 (37) | 165 (63) | 99 (37,8) | 163 (62,2) |
Основная сложность классификации пациенток с кальцинатами заключалась в том, что доля женщин с несосудистыми кальцинатами достаточна мала по сравнению с пациентками, у которых отмечали любой тип кальцинатов (табл. 7).
Таблица 7. Распределение пациенток по типу кальцинатов для левой и правой молочной железы | ||||
Молочная железа | Отсутствие кальцинатов, n (%) | Несосудистые кальцинаты (тип 1), n (%) | Сосудистые кальцинаты (тип 2), n (%) | Сосудистые и несосудистые кальцинаты (тип 3), n (%) |
Левая | 315 (30,6) | 55 (5,3) | 518 (50,3) | 142 (13,8) |
Правая | 316 (30,7) | 61 (5,9) | 515 (50) | 138 (13,4) |
Следует отметить, что при разделении на 10 групп у женщин с высокой рентгенологической плотностью молочных желёз отсутствовала классификация по типу кальцинатов, однако было разделение по числу вовлечённых квадрантов.
Кроме того, отмечена малочисленность групп G1 и G4, с чем связаны высокие ОШ и широкие ДИ для них. Именно поэтому мы решили объединить группу G4 с группой G3 в одну, а G1 перераспределить: пациенток с одним вовлечённым квадрантом отнести к группе G2, а с двумя и более — к G3.
Таким образом, мы получили восемь новых непересекающихся групп (см. табл. 1, 2). При такой классификации у женщин с высокой плотностью молочных желёз отсутствует разделение по типу кальцинатов, однако остаётся разделение по числу вовлечённых квадрантов. На рис. 12 продемонстрированы значения ОШ на графике в логарифмической шкале.

Рис. 12. Отношение шансов с 95% доверительным интервалом для каждой из семи полученных групп (G1–G7) по сравнению с референсом G0 в логарифмической шкале по основанию два: a — левая молочная железа; b — правая молочная железа.
ОБСУЖДЕНИЕ
Резюме основного результата исследования
Представлены результаты математического анализа факторов риска развития ССЗ у пациенток в зависимости от рентгенологической плотности молочной железы, наличия кальцинатов и их распространённости. Установлено, что у женщин с низкой рентгенологической плотностью молочных желёз (ACR A или B) и сосудистыми кальцинатами, выявленными более чем в одном квадранте, вероятность определения высокой и очень высокой категории риска ССЗ превышает 75%. В свою очередь, при сочетании сосудистых и несосудистых кальцинатов в двух и более квадрантов вероятность отнесения к данным категориям риска превышает 90%.
Интерпретация результатов исследования
Результаты настоящего исследования демонстрируют, что помимо общепринятых факторов риска ССЗ, большое значение для женской популяции имеют рентгенологические характеристики плотности молочной железы и степень выраженности кальциноза. Полученные данные подчёркивают необходимость комплексной оценки стандартных клинических факторов риска совместно с рентгенологическими характеристиками, позволяя повысить точность стратификации риска и своевременно выявить женщин с высокой и очень высокой категории риска ССЗ в соответствии со шкалой SCORE2, что согласуется с результатами, полученными E. Aldous и соавт. [9]. Авторы установили, что наличие кальцинатов молочных артерий и низкой рентгенологической плотности молочной железы, как по отдельности, так и в сочетании, ассоциированы с ишемической болезнью сердца и улучшают прогнозирование риска в сравнении со стандартной оценкой риска ССЗ. Это подчёркивает необходимость комплексного подхода и целесообразность создания единых алгоритмов оценки. Тем не менее в большинстве ранее проведённых исследований не рассматривали совместное влияние рентгенологической плотности молочных желёз и наличия кальцинатов, включая их тип и распространённость, на риск ССЗ [6–8].
В свою очередь, для оценки категории риска развития ССЗ важно учитывать наличие не только сосудистых кальцинатов, но и их сочетание с несосудистыми. Сосудистые кальцинаты имеют характерные признаки и на маммограммах они визуализируются как параллельные гиперденсные линии, повторяющие ход стенок сосудов. Их также называют кальцинатами Менкеберга, расположенными в среднем слое (медии) сосудистой стенки (рис. 13) [13, 14]. К несосудистым кальцинатам относят микрокальцинаты — отложения кальция в ткани молочной железы размером менее 0,5 мм. В большинстве случаев они имеют доброкачественный характер и их выявляют примерно у половины обследуемых женщин. Полагают, что микрокальцификация ассоциирована с отложением соединений с высоким содержанием кальция, возникающих в результате различных физиологических и патофизиологических процессов: секреторных, воспалительных, инволютивных, а также вследствие травматизации или некроза1. Кроме того, выделяют внутрикожные микрокальцинаты, локализованные преимущественно в дерме и обусловленные обызвествлением протоков сальных желёз. Обычно они группируются и имеют кольцевидную или точечную форму (рис. 14). Для фиброзно-кистозных изменений характерны кальцинаты по типу Weddell, имеющие квадратную, треугольную или трапецивидную форму (рис. 15). Округлые кальцинаты с просветлением в центре, а также по типу «яичной скорлупы» встречают при обызвествлении макро- и микрокист (рис. 16). Для мелких кист молочной железы типичны кальцинаты по типу «молочка кальция», формирующиеся вследствие седиментации кальция в полости кисты и имеющие форму чашечки или полумесяца в боковой проекции (рис. 17). Множественные рассеянные точечные микрокальцинаты характерны для склерозирующего аденоза — доброкачественного состояния, сопровождающегося увеличение долек железистой ткани и их сдавлением фиброзным компонентом [13] (рис. 18). Глыбчатые микрокальцинаты с множественными просветами внутри наблюдают при обызвествлении папиллом молочной железы (рис. 19). Линейные и стержневидные кальцинаты, ориентированные вдоль протоков, формируются при инфильтрации перидуктальной стромы плазматическими клетками и пролиферации базального слоя, что является патогномоничным признаком перенесённого плазмоклеточного мастита (рис. 20).

Рис. 13. Кальциноз стенок артерий молочной железы.

Рис. 14. Внутрикожные микрокальцинаты.

Рис. 15. Кальцинаты по типу Weddell.

Рис. 16. Обызвествление мелкой киста молочной железы.

Рис. 17. Кальцинат по типу «чашечки».

Рис. 18. Множественные точечные микрокальцинаты при склерозирующем аденозе.

Рис. 19. Обызвествление папилломы в структуре молочной железы.

Рис. 20. Рентгенологическая картина перенесённого плазмоклеточного мастита: линейные кальцинаты по ходу млечных протоков.
Важным параметром, ассоциированным с риском ССЗ, является количество квадрантов, в которых выявляют кальцинаты. При анализе их наличия и распределения в одной молочной железе точность связи с категорией риска ССЗ статистически значимо не снижается, однако трудоёмкость определения рентгенологических характеристик уменьшается в 2 раза.
Мы считаем, что одним из важных аспектов использования полученных данных в качестве рентгенологических маркёров риска ССЗ является возможность их интеграции в скрининговые программы с использованием технологий искусственного интеллекта. Это особенно важно в связи с субъективностью оценки рентгенологической плотности молочных желёз и выраженностью их кальциноза, которая в значительной степени зависит от опыта рентгенологов. По нашему мнению, программы, позволяющие автоматизировано оценивать рентгенологическую плотность молочной железы, наличие и выраженность кальциноза, могут существенно повысить объективность и воспроизводимость диагностики, а также стандартизировать интерпретацию данных.
Необходимо продолжить исследование, направленное на более детальное изучение связь между сосудистыми кальцинатами в молочной железе, её рентгенологической плотностью и категорией риска ССЗ.
Ограничения исследования
В данном исследовании не оценивали частоту развития сердечно-сосудистых событий.
Кроме того, к ограничениям нашего исследования относятся сравнительно небольшая выборка и неравномерное формирование обследуемых групп по численности.
В связи с тем, что при планировании и проведении исследования размер выборки для достижения требуемой статистической мощности результатов не рассчитывали, полученную выборку участниц невозможно считать в достаточной степени репрезентативной, что не позволяет экстраполировать полученные результаты и их интерпретацию на генеральную совокупность аналогичных пациентов за пределами исследования.
ЗАКЛЮЧЕНИЕ
Таким образом, результаты настоящего исследования подтверждают наличие взаимосвязи между рентгенологической плотностью молочной железы, выраженностью кальциноза её артерий и риском развития сердечно-сосудистых событий.
Применение методов машинного обучения в сочетании со статистическим анализом позволило разделить пациенток на ранжированные группы. В то же время текущее количество выделенных групп остаётся достаточно большим, что затрудняет применение этой информации в клинической практике. Однако полученные результаты могут послужить основой для дальнейшей систематизации и разработки удобного алгоритма принятия решений по маршрутизации пациенток.
По нашему мнению, использование сочетанных данных о рентгенологической плотности молочной железы и выраженности кальциноза её артерий является перспективным направлением для прогнозирования категории риска ССЗ. Данный подход обладает потенциалом для улучшения диагностики и профилактики ССЗ.
С учётом того, что маммография уже является стандартным методом скрининга рака молочной железы, добавление оценки рентгенологической плотности молочной железы и кальциноза её артерий в программу анализа результатов может обеспечить более широкий спектр информации о состоянии здоровья женщин, не требуя при этом дополнительных затрат.
ДОПОЛНИТЕЛЬНАЯ ИНФОРМАЦИЯ
Вклад авторов. Д.Д. Цурская — концепция и дизайн исследования, сбор и анализ литературных данных, анализ маммограмм, написание и редактирование текста рукописи, подготовка графических материалов; Е.А. Мершина — концепция и дизайн исследования, сбор и анализ литературных данных, анализ маммограмм, редактирование текста рукописи; В.Е. Синицын — концепция и дизайн исследования, анализ литературных данных, редактирование текста рукописи; O.Е. Ивлев — анализ литературных данных, применение методов машинного обучения, статистический анализ данных, редактирование текста рукописи; Е.М. Филичкина — сбор и анализ литературных данных, вероятностно-статистический анализ, написание и редактирование текста рукописи; Е.Б. Яровая — концепция и дизайн исследования, анализ литературных данных, вероятностно-статистический анализ, редактирование текста рукописи; Г.О. Долгушин, Я.А. Орлова — формирование базы пациентов, сбор и анализ литературных данных, редактирование текста рукописи. Все авторы одобрили рукопись (версию для публикации), а также согласились нести ответственность за все аспекты настоящей работы, гарантируют надлежащее рассмотрение и решение вопросов, связанных с точностью и добросовестностью любой её части.
Этическая экспертиза. Протокол исследования одобрен локальным этическим комитетом Медицинского научно-образовательного центра Московского государственного университета имени М.В. Ломоносова (Протокол № 5 от 16.10.2023).
Источники финансирования. Работа проведена по государственному заданию в рамках междисциплинарных научных проектов исследовательских коллективов Московского государственного университета имени М.В. Ломоносова, выполняющихся в интересах Междисциплинарных научно-образовательных школ Московского университета. Проект № 23-Ш05-08 «Интегральный метод оценки сердечно-сосудистого риска с привлечением данных лучевой диагностики молочных желёз на основе вероятностно-статистических моделей».
Раскрытие интересов. Авторы заявляют об отсутствии отношений, деятельности и интересов за последние три года, связанных с третьими лицами (коммерческими и некоммерческими), интересы которых могут быть затронуты содержанием статьи.
Оригинальность. При создании настоящей работы авторы не использовали ранее опубликованные сведения (текст, иллюстрации, данные).
Доступ к данным. Редакционная политика в отношении совместного использования данных к настоящей работе не применима.
Генеративный искусственный интеллект. При создании настоящей статьи технологии генеративного искусственного интеллекта не использовали.
Рассмотрение и рецензирование. Настоящая работа подана в журнал в инициативном порядке и рассмотрена по обычной процедуре. В рецензировании участвовали три внешних рецензента, и член редакционной коллегии журнала.
ADDITIONAL INFORMATION
Author contributions: D.D. Tsurskaya: conceptualization, methodology, investigation, formal analysis, writing—original draft, writing—review & editing, visualization; E.A. Mershina: conceptualization, methodology, investigation, formal analysis, writing—review & editing; V.E. Sinitsyn: conceptualization, methodology, investigation, writing—review & editing; O.E. Ivlev: investigation, software, formal analysis, writing—review & editing; E.M. Filichkina: investigation, formal analysis, writing—original draft, writing—review & editing, visualization; E.B. Yarovaya: conceptualization, methodology, formal analysis, writing—review & editing; G.O. Dolgushin, Ia.A. Orlova: resources, investigation, writing—review & editing. All the authors approved the version of the manuscript to be published and agreed to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethics approval: The study protocol was approved by the local Ethics Committee of the Medical Research and Educational Center Moscow at the Lomonosov Moscow State University (Minutes No. 5, dated October 16, 2023).
Funding sources: The work was performed by the university’s research teams as part of Moscow State University’s interdisciplinary research project under a state assignment in the interest of the University’s Interdisciplinary Research and Educational Schools. Project No. 23-Sh05-08: An Integrated Method for Assessing Cardiovascular Risk Using Mammography-Based Probabilistic Models.
Disclosure of interests: The authors have no relationships, activities, or interests for the last three years related to for-profit or not-for-profit third parties whose interests may be affected by the content of the article.
Statement of originality: No previously obtained or published material (text, images, or data) was used in this study or article.
Data availability statement: The editorial policy regarding data sharing does not apply to this work.
Generative AI: No generative artificial intelligence technologies were used to prepare this article.
Provenance and peer-review: This article was submitted unsolicited and reviewed following the standard procedure. The peer review process involved three external reviewers and a member of the Editorial Board.
1 Udoh AI, He J. Microcalcifications [Internet]. В: PathologyOutlines.com. Режим доступа: https://www.pathologyoutlines.com/topic/breastcalcification.html Режим доступа: 22.12.2024.
About the authors
Daria D. Tsurskaya
Lomonosov Moscow State University
Author for correspondence.
Email: dashnom03@gmail.com
ORCID iD: 0009-0008-7732-4093
SPIN-code: 5298-8707
MD
Russian Federation, MoscowElena A. Mershina
Lomonosov Moscow State University
Email: elena_mershina@mail.ru
ORCID iD: 0000-0002-1266-4926
SPIN-code: 6897-9641
MD, Cand. Sci. (Medicine), Assistant Professor
Russian Federation, MoscowValentin E. Sinitsyn
Lomonosov Moscow State University
Email: vsini@mail.ru
ORCID iD: 0000-0002-5649-2193
SPIN-code: 8449-6590
MD, Dr. Sci. (Medicine), Professor
Russian Federation, MoscowOleg E. Ivlev
Lomonosov Moscow State University
Email: oleg.ivlev@math.msu.ru
ORCID iD: 0000-0002-3663-6305
SPIN-code: 8257-0252
Russian Federation, Moscow
Elena M. Filichkina
Lomonosov Moscow State University
Email: elena.filichkina1999@yandex.ru
ORCID iD: 0000-0003-3715-6896
SPIN-code: 3153-4281
Russian Federation, Moscow
Elena B. Yarovaya
Lomonosov Moscow State University
Email: yarovaya@mech.math.msu.su
ORCID iD: 0000-0002-6615-4315
SPIN-code: 5591-8439
Dr. Sci. (Physics and Mathematics)
Russian Federation, MoscowGrigory O. Dolgushin
Lomonosov Moscow State University
Email: grdolgushin@yandex.ru
ORCID iD: 0000-0002-5981-3933
SPIN-code: 3452-9799
MD
Russian Federation, MoscowIana А. Orlova
Lomonosov Moscow State University
Email: 5163002@bk.ru
ORCID iD: 0000-0002-8160-5612
SPIN-code: 3153-8373
MD, Dr. Sci. (Medicine), Professor
Russian Federation, MoscowReferences
- US Preventive Services Task Force; Nicholson WK, Silverstein M, Wong JB, et al. Screening for Breast Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2024;331(22):1918–1930. doi: 10.1001/jama.2024.5534
- Guidelines for the Prevention of Breast Cancer [Internet]. Moscow: Ministry of Health of the Russian Federation; 2018. [cited 2024 Dec 22]. Available from: https://ncagp.ru/upload/files/docs/RMJ_moloch.pdf?ysclid=mewsn371hm639990283
- Minssen L, Dao TH, Quang AV, et al. Breast Arterial Calcifications on Mammography: A New Marker of Cardiovascular Risk in Asymptomatic Middle Age Women? European Radiology. 2022;32(7):4889–4897. doi: 10.1007/s00330-022-08571-3 EDN: RQELYA
- Bochkareva EV. Kim IV, Butina EK, et al. Mammographic Screening as a Tool for Cardiovascular Risk Assessing. Part 2. Association of Breast Arterial Calcification and Cardiovascular Diseases. Rational Pharmacotherapy in Cardiology. 2019;15(3):424–430. doi: 10.20996/1819-6446-2019-15-3-424-430 EDN: VDJPIL
- Bazhenova DA, Puchkova OS, Mershina EA, Sinitsyn VE. Evaluation of Breast Vascular Calcifications as a Predictor for Coronary Artery Calcification. Journal of Radiology and Nuclear Medicine. 2021;102(3):196–202. doi: 10.20862/0042-4676-2021-102-3-196-202 EDN: WXGNDW
- Bui QM, Daniels LB. A Review of the Role of Breast Arterial Calcification for Cardiovascular Risk Stratification in Women. Circulation. 2019;139(8):1094–1101. doi: 10.1161/CIRCULATIONAHA.118.038092
- Bochkareva EV, Rozhkova NI, Butina E. K EK, et al. Mammographic Breast Density and Cardiovascular Disease in Women. A Literature Review. Cardiovascular Therapy and Prevention. 2024;23(8):126–133. doi: 10.15829/1728-8800-2024-4064 EDN: HHWMOF
- Sardu C, Gatta G, Pieretti G, et al. Pre-Menopausal Breast Fat Density Might Predict MACE During 10 Years of Follow-Up. JACC: Cardiovascular Imaging. 2021;14(2):426–438. doi: 10.1016/j.jcmg.2020.08.028 EDN: OAOFKF
- Aldous E, Goel V, Cameron W, et al. Combined Mammographic Breast Density and Breast Arterial Calcification as an Incremental Predictor of Coronary Artery Disease. Journal of Women's Health. 2025;34(7):889–896. doi: 10.1089/jwh.2024.0966 EDN: NKOLFQ
- D'Orsi CJ, Sickles EA, Mendelson EB, Morris EA. ACR BI-RADS Atlas: Breast Imaging Reporting and Data System. Reston: American College of Radiology; 2013. ISBN: 9781559030168 Available from: https://books.google.ru/books?id=nhWSjwEACAAJ&hl
- Boytsov SA, Pogosova NV, Ansheles AA, et al. Cardiovascular Prevention 2022. Russian National Guidelines. Russian Journal of Cardiology. 2023;28(5):119–249. doi: 10.15829/1560-4071-2023-5452 EDN: EUDWYG
- McInnes L, Healy J, Melville J. UMAP: Uniform Manifold Approximation and Projection for Dimension Reduction. arXiv. 2018. doi: 10.48550/arXiv.1802.03426
- Ali EA, Fouad H, Razek NA, et al. Evaluation of Mammography Detected Breast Arterial Calcifications as a Predictor of Coronary Cardiac Risk. Egyptian Journal of Radiology and Nuclear Medicine. 2019;50(1):81. doi: 10.1186/s43055-019-0095-7
- Bell BM, Gossweiler M. Benign Breast Calcifications. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557567/
Supplementary files

