

")





Multiple biliary microhamartomas diagnosed in an unsuspecting elderly patient
- Autores: Balbino M.1, Montatore M.1, Fascia G.1, Tupputi R.2, Masino F.1, Muscatella G.1, Mannatrizio D.1, Guglielmi G.1,2,3
-
Afiliações:
- University of Foggia
- Dimiccoli Hospital
- Casa Sollievo della Sofferenza Hospital
- Edição: Volume 5, Nº 2 (2024)
- Páginas: 334-341
- Seção: Case reports
- ##submission.dateSubmitted##: 14.11.2023
- ##submission.dateAccepted##: 19.12.2023
- ##submission.datePublished##: 20.09.2024
- URL: https://jdigitaldiagnostics.com/DD/article/view/623322
- DOI: https://doi.org/10.17816/DD623322
- ID: 623322

Citar

Resumo
Multiple biliary hamartomas are a benign incidental finding in the liver. They are not easily detected if one has never seen them, and if appropriate imaging tests are unavailable, and also can be challenging to differentiate from other liver lesions based on imaging alone. Thus, this study aimed to expand the radiologist’s digital image library, enabling a quick and precise differential diagnosis. This paper also highlights the importance of thorough radiological assessment and need for a multidisciplinary approach, involving radiologists, hepatologists, and pathologists, to ensure a precise diagnosis.
The patient presented at the hospital for a computed tomography scan and an abdominal magnetic resonance imaging recommended by his general practitioner to assess the biliary tree (magnetic resonance cholangiopancreatography), owing to persistent abdominal pain. The patient had never undergone an abdominal magnetic resonance imaging previously; hence, the discovery of hepatic lesions was incidental and unexpected.
Magnetic resonance imaging revealed multiple benign lesions in both the hepatic lobes comparable to the Von Meyenburg complex. These lesions are multiple hamartomas and behave differently in all magnetic resonance imaging sequences.
Images acquired with different magnetic resonance imaging sequences were carefully examined. Multiple lesions were found scattered throughout the liver; however, the lesions were benign and consistent with the diagnosis of multiple biliary hamartomas.
Medical practitioners should examine the presence of multiple biliary hamartomas and consider them in the differential diagnosis when patients present with hepatic abnormalities. This can prevent unnecessary interventions and guide appropriate patient management.
Texto integral
INTRODUCTION
Multiple biliary hamartomas are relatively rare and often an incidental finding during imaging studies. Identifying and accurately diagnosing these lesions are crucial because they can mimic other hepatic lesions, such as cysts or tumors, leading to potentially unnecessary invasive procedures or treatments [1-4].
DESCRIPTION OF THE CASE
Medical History
An 82-year-old male presented to the hospital with a primary complaint of abdominal pain persisting for more than 6 weeks. The patient has no personal/family history significant for liver disease. A thorough medical evaluation, including physical examination and blood tests, was conducted. However, these initial assessments did not yield conclusive results nor provide a clear diagnosis.
Diagnostic Assessment
The patient underwent contrast-enhanced CT (computed tomography) and subsequently MRI [5–6].
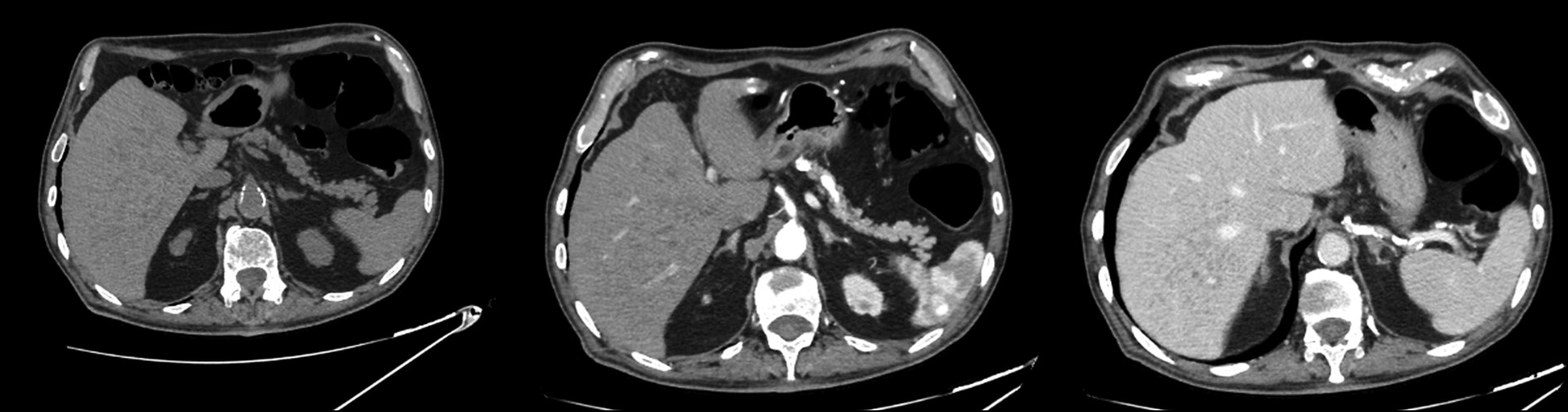
Multiple millimetric disorganized hypodense lesions, both subcapsular and intraparenchymal, were detected incidentally in both hepatic lobes on CT.
After the administration of contrast medium, enhancement of lesions was not observed (Fig. 1).

Fig. 1. Axial CT image: hypodense lesions without significant contrast enhancement in the arterial and venous phases.
Subsequent MRI examination identified the same lesions with different characteristics in various sequences. In T2-weighted MRI images, the areas appear homogeneously and intensely hyperintense (Fig. 2).

Fig. 2. Coronal and axial MRI images with HASTE T2 sequence: multiple small hyperintense lesions throughout the hepatic area.
In T1-weighted images, all the lesions were homogeneously hypointense.
In diffusion-weighted imaging (DWI), the lesions persist as hyperintense at a low B-value (50 sec/mm2) but disappear at a high B-value (800) (Fig. 3).

Fig. 3. Axial MRI image with DWI sequence: hyperintense lesions at low B-value (50 sec/mm2) on the right, disappearing at high B-values on the left (800).
In T2-weighted MRI–cholangiography sequences, the liver presents a “starry sky” appearance due to the presence of multiple small hyperintense lesions; however, the communication with the bile duct are usually not recognized [7] (Fig. 4).

Fig. 4. MRI image with T2 MRI–cholangiography sequence: multiple small hyperintense lesions; the liver with a “starry sky” appearance.
The dynamic study after contrast administration did not show enhancement in the arterial and venous phases (Fig. 5).

Fig. 5. Axial MRI image with T1 sequence showing hypointense lesions without significant contrast enhancement in the arterial and venous phases.
Differential Diagnosis
Radiographic findings may be nonspecific and may not differentiate biliary hamartomas from other lesions.
The differential diagnosis is made with polycystic liver disease, multiple simple hepatic cysts, metastases, micro-abscesses, and Caroli’s disease [8]. A more heterogeneous appearance of lesions and communication with the bile duct is observed in the latter.
Interventions
In the present case, the lesions were not directly related to symptoms or complications therefore, no surgical or pharmacological treatment was required.
If Von Meyenburg complexes are causing symptoms or complications, treatment may include surgical removal of the affected liver tissue or drainage of large cysts [9–11].
It is critical for individuals diagnosed with these complexes to consult a hepatologist or liver specialist to determine the appropriate management approach based on their specific case.
Follow-up and Outcomes
The management of the patient’s condition was based on observation and scheduled monitoring, allowing for the timely assessment of any potential alterations. However, no significant changes led to alterations in the diagnostic choices made.
DISCUSSION
Multiple biliary hamartomas, also called Von Meyenburg complexes, are rare benign liver lesions characterized by small disorganized cystic structures affecting both hepatic lobes with some predilection for subcapsular regions [12–13]. They are multiple small round, or irregular lesions and are usually 5–30 mm in size on imaging.
These structures are composed of abnormal bile ducts and are typically discovered incidentally during medical imaging studies, such as ultrasound, CT, and MRI, which are often performed for other reasons. Although hamartomas can communicate with the biliary tree, but usually not. They are believed to arise from embryonic bile duct remnants that have failed to involute.
Von Meyenburg complexes are considered noncancerous and are usually asymptomatic. They are generally not associated with liver dysfunction or clinical symptoms. Laboratory data are generally nonspecific and within normal limits. Most individuals with these lesions do not require treatment. In some cases, Von Meyenburg complexes can be associated with various liver conditions, including polycystic liver disease, Caroli’s disease, and congenital hepatic fibrosis [14].
When these conditions are present, they can lead to more significant liver-related problems and may require medical management.
CONCLUSION
Von Meyenburg complexes a rare medical condition that is often detected incidentally. This study highlights the importance of accurate diagnosis and challenges in distinguishing these lesions from other hepatic lesions. Management based on observation and periodic monitoring is a feasible approach when the lesions are asymptomatic. However, clinical awareness on multiple biliary hamartomas is crucial to avoid misdiagnosis and unnecessary invasive interventions. Future studies may further our understanding of this condition and its clinical implications.
ADDITIONAL INFORMATION
Funding source. This study was not supported by any external sources of funding.
Competing interests. The authors declare that they have no competing interests.
Authors’ contribution. All authors made a substantial contribution to the conception of the work, acquisition, analysis, interpretation of data for the work, drafting and revising the work, final approval of the version to be published and agree to be accountable for all aspects of the work.
Consent for publication. Written consent was obtained from the patient for publication of relevant medical information and all of accompanying images within the manuscript in Digital Diagnostics Journal.
Sobre autores
Marina Balbino
University of Foggia
Email: marinabalbino93@gmail.com
ORCID ID: 0009-0009-2808-5708
MD
Itália, FoggiaManuela Montatore
University of Foggia
Email: manuela.montatore@unifg.it
ORCID ID: 0009-0002-1526-5047
MD
Itália, FoggiaGiacomo Fascia
University of Foggia
Email: giacomo.fascia@unifg.it
ORCID ID: 0000-0001-5244-5093
MD
Itália, FoggiaRuggiero Tupputi
Dimiccoli Hospital
Email: rutudott@gmail.com
MD
Itália, BarlettaFederica Masino
University of Foggia
Email: federicamasino@gmail.com
MD
Itália, FoggiaGianmichele Muscatella
University of Foggia
Email: muscatella94@gmail.com
ORCID ID: 0009-0004-3535-5802
MD
Itália, FoggiaDomenico Mannatrizio
University of Foggia
Email: dr.mannatrizio@gmail.com
ORCID ID: 0000-0003-3365-7132
Itália, Foggia
Giuseppe Guglielmi
University of Foggia; Dimiccoli Hospital; Casa Sollievo della Sofferenza Hospital
Autor responsável pela correspondência
Email: giuseppe.guglielmi@unifg.it
ORCID ID: 0000-0002-4325-8330
MD, Professor
Itália, Foggia; Barletta; FoggiaBibliografia
- Zheng RQ, Zhang B, Kudo M, Onda H, Inoue T. Imaging findings of biliary hamartomas. World J Gastroenterol. 2005;11(40):6354–6359. doi: 10.3748/wjg.v11.i40.6354
- Gil-Bello D, Ballesteros E, Sanfeliu E, Andreu FJ. Calcification in biliary hamartomatosis. Br J Radiol. 2012;85(1012):e099–e101. doi: 10.1259/bjr/95019559
- Thommesen N. Biliary hamartomas (von Meyenburg complexes) in liver needle biopsies. Acta Pathol Microbiol Scand A. 1978;86(2):93–99. doi: 10.1111/j.1699-0463.1978.tb02019.x
- Aguado IC, Álvarez MH, Hernández JS, La Orden Izquierdo E. Hamartomatosis biliar en una lactante con colitis alérgica: revisión a propósito de un caso. Rev Pediatr Aten Primaria. 2013;15(59):e111–e114. doi: 10.4321/S1139-76322013000400014
- Horton KM, Bluemke DA, Hruban RH, Soyer P, Fishman EK. CT and MR imaging of benign hepatic and biliary tumors. Radiographics. 1999;19(2):431–451. doi: 10.1148/radiographics.19.2.g99mr0443
- Brancatelli G, Federle MP, Vilgrain V, et al. Fibropolycystic liver disease: CT and MR imaging findings. RadioGraphics. 2005;25(3):659–670. doi: 10.1148/rg.253045114
- Bravo-Acosta M, Rosendo-Namías J, Martínez-Méndez D. Hamartomatosis biliar múltiple: “imagen en cielo estrellado”. Rev Gastroenterol MEX. 2020;86(2). doi: 10.1016/j.rgmx.2020.08.002
- Choi BI, Yeon KM, Kim SH, et al. Caroli disease: central dot sign in CT. Radiology. 1990;174(1):161–163. doi: 10.1148/radiology.174.1.2294544
- Kin HK, Jin SY. Cholangiocarcinoma arising in von Meyenburg complexes. Korean J Hepatol. 2011;17(2):161–164. doi: 10.3350/kjhep.2011.17.2.161
- Song JS, Lee YJ, Kim KW, et al. Cholangiocarcinoma arising in von Meyenburg complexes: report of four cases. Pathol Int. 2008;58(8):503–512. doi: 10.1111/j.1440-1827.2008.02264.x
- Xu AM, Xian ZH, Zhang SH, Chen XF. Intrahepatic cholangiocarcinoma arising in multiple bile duct hamartomas: report of two cases and review of the literature. Eur J Gastroenterol Hepatol. 2009;21(5):580–584. doi: 10.1097/MEG.0b013e3282fc73b1
- Venkatanarasimha N, Thomas R, Armstrong EM, et al. Imaging features of ductal plate malformations in adults. Clin Radiol. 2011;66(11):1086–1093. doi: 10.1016/j.crad.2011.05.008
- Desmet VJ. Pathogenesis of ductal plate malformation. J Gastroenterol Hepatol. 2004;19(S7):S356–S360. doi: 10.1111/j.1440-1746.2004.03702.x
- Soreide K, Korner H, Havnen J, et al. Bile duct cysts in adults. Br J Surg. 2004;91(12):1538–1548. doi: 10.1002/bjs.4815
Arquivos suplementares

