

")





Unilateral isolated fracture of the pterygoid plate: a case report
- Autores: Balzano R.F.1, Testini V.2, Cammarota A.3, Guglielmi G.1,2,4
-
Afiliações:
- Radiology Unit, Barletta University Campus UNIFG, “Dimiccoli” Hospital
- Department of Clinical and Experimental Medicine, Foggia University School of Medicine
- Radiation Oncology Unit, IRCCS CROB, Rionero in Vulture
- Radiology Unit, Hospital “Casa Sollievo Della Sofferenza”, San Giovanni Rotondo
- Edição: Volume 3, Nº 1 (2022)
- Páginas: 71-77
- Seção: Case reports
- ##submission.dateSubmitted##: 13.12.2021
- ##submission.dateAccepted##: 01.02.2022
- ##submission.datePublished##: 24.04.2022
- URL: https://jdigitaldiagnostics.com/DD/article/view/90282
- DOI: https://doi.org/10.17816/DD90282
- ID: 90282

Citar

Resumo
Pterygoid plate fractures are often associated with Le Fort fractures and accompanied by other facial fractures such as frontal sinus and naso-orbital-ethmoid fractures; isolated pterygoid plate fractures are extremely rare.
Le Fort fractures must be surgically treated with fixation of unstable fracture segments to re-establish bone form and function, and the pterygoid process must be surgically stabilized; however, surgical treatment is unnecessary in isolated pterygoid plate fractures.
Here, we report a rare case of isolated unilateral fracture of the pterygoid process in a 71-year-old female patient who had a syncopal episode with secondary head injury and a hematoma at the base of the right orbit.
A computed tomography scan showed unilateral right pterygoid plate fracture with signs of emphysema in the ipsilateral masticatory space. The patient also had a fracture of the medial wall of the right maxillary sinus with hemosine, but no fractures of the skull base or theca. She was treated conservatively.
Palavras-chave
Texto integral
BACKGROUND
Pterygoid plate fractures are usually associated with all Le Fort midface fractures (Le Fort I, II, and III, according to the plane of injury).
Isolated fractures of the pterygoid plate are extremely rare. Herein, we present a case of an isolated fracture of the right pterygoid plate in an adult female.
DESCRIPTION OF THE CASE
A 71-year-old female patient presented to the emergency department for an head injury secondary to a syncopal episode with a consequent fall to the ground. Her general physical examination results were unremarkable. No facial palsy was observed. Previous medical and surgical histories were noncontributory and she had not been unconscious.
The patient exhibited a marked swelling of the right side of the face and had a hematoma at the base of the right orbit. The skin of the right cheek and zygomatic region displayed some degree of paresthesia.
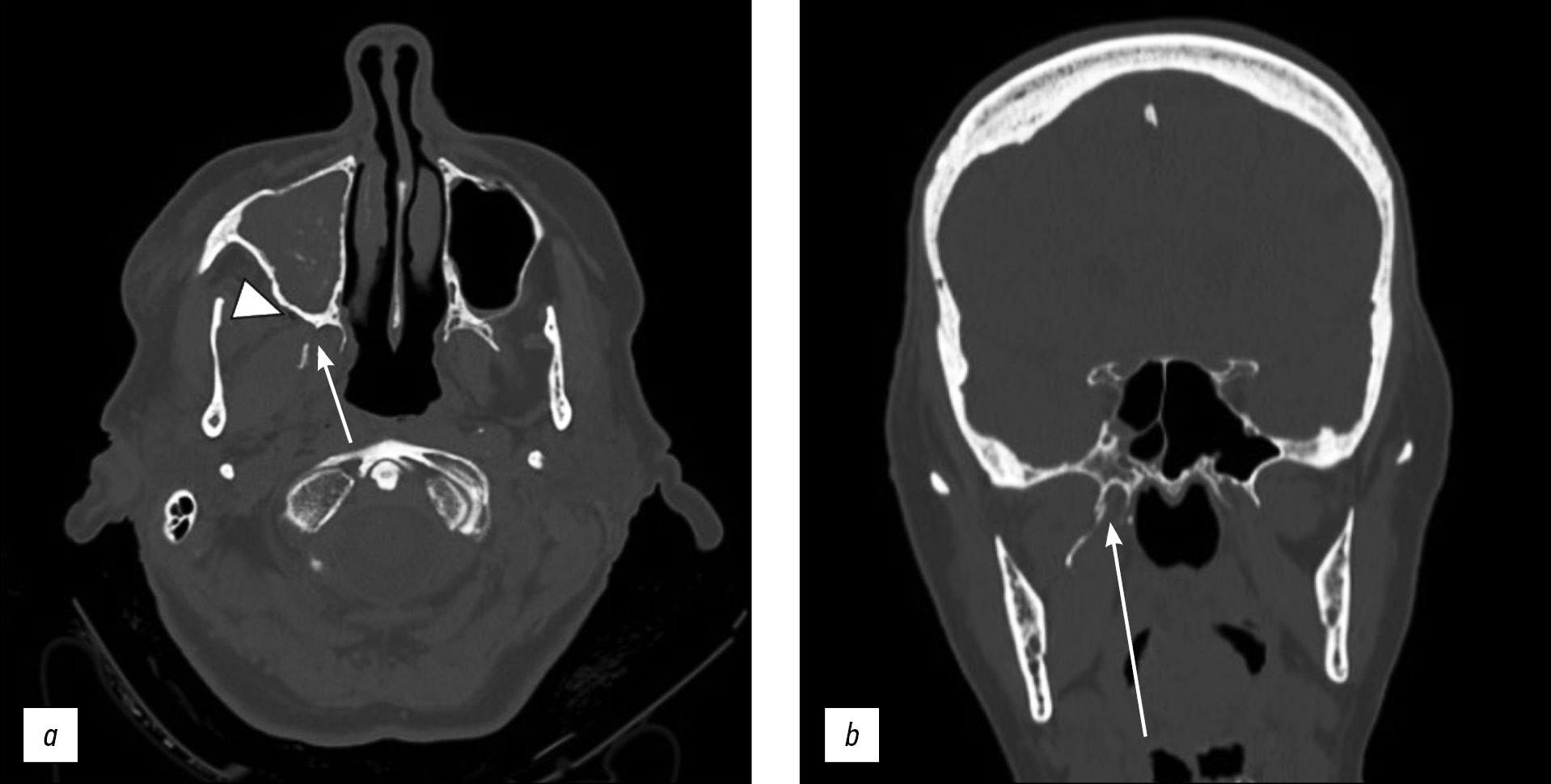
The patient was referred to the radiology department for noncontrast-enhanced high-resolution computed tomography (CT) on a 64-slice scanner, which showed unilateral right pterygoid plate fracture with signs of emphysema in the ipsilateral masticatory space (Fig. 1a, 1b). The CT investigation also documented the fracture of the medial wall of the right maxillary sinus with hemosine (Fig. 2a, 2b, 2c).

Fig 1: Axial (a) and coronal (b) CT scan with a bone window showing unilateral right pterygoid plate fracture (arrows) with air bubbles of emphysema (arrowheads) in the ipsilateral masticatory space.

Fig 2: Axial (a) and coronal (b) CT scan with bone window documents the fracture of the medial wall of the right maxillary sinus (arrows). Soft window (c) shows hemosine in the right maxillary sinus (arrowhead).
Fractures of the skull base or theca were not evident, nor were there any changes in the cerebral nerve tissue density. Surgery treatment was unnecessary.
DISCUSSION
The main causes of facial fractures are motor vehicular accidents, assaults, falls, sports injuries, gun-shot injuries, etc [1].
Knowledge of the musculoskeletal system of the facial skeleton is important for diagnosing facial fractures. In practice, between the buttresses of the face that represent the areas of relatively increased bone thickness that support the functional units of the face, the posterior maxillary buttress is found, which is a bone column at the pterygomaxillary junction [2], a site of several fracture types, including the Le Fort fractures, as first described in 1901 [3].
These fractures are classified into 3 distinct groups based on the fracture direction as horizontal, pyramidal, or transverse.
The Le Fort I fracture involves the nasal cavity anterolateral margin. This type of fracture may result from a force directed in a downward direction against the upper teeth.
In Le Fort II fractures, the fracture line extends to the lower orbital margins, which results from a force to the lower or mid maxilla.
The Le Fort III fractures involve the zygomatic arch and are caused by the nasal bridge and upper maxilla impact [4].
The pterygoid plate is involved in all types of Le Fort fractures and may result in a pterygomaxillary separation [5]. Le Fort fractures are often associated with other facial fractures, such as frontal sinus fractures, and with naso-orbital-ethmoid fractures [6].
Isolated pterygoid plate fractures are extremely rare. The study of Garg et al. [7] revealed that approximately two-thirds of patients with pterygoid plate fractures had an associated Le Fort fracture. Therefore, fractures of the pterygoid plate do not necessarily equate to the presence of a Le Fort fracture. Pterygoid plate fractures are often an extension of the skull base and vault fractures or the likely consequence of impingement caused by a displaced mandible fracture [7]. In 2014, Anh Q. Truong et al. [8] described an association between lateral pterygoid plate fractures and mandibular fractures. A retrospective study by Garg et al. [7] revealed that 78 patients (just over a third) did not have Le Fort fractures out of 209 patients with pterygoid plate fractures, whereas other fractures were found in these patients, such as fractures of the sphenotemporal buttress, temporal bone, and zygomatic–maxillary complex, and displaced mandibular fractures. Similar results have been reported from other studies [9].
In 2017, Surya [6] described a case of an isolated fracture of the pterygoid plate caused by a foreign body penetration.
There are several mechanisms of injury to the pterygoid plate by a direct traumatic force (penetrating trauma) or indirect (traction of the pterygoid muscle) that propagate along with the areas of weakness within the facial structures. In sphenotemporal buttress fractures, connections with the temporal, zygomatic, and sphenoid bones are lost and the fracture line extends to the pterygoid plate [8].
Pterygoid plaques are the site of origin of the medial and lateral pterygoid muscles, [10] thus any trauma to the pterygoid plaques could potentially cause discomfort with chewing, jaw movement, and speech.
Le Fort fractures must be surgically treated after stabilizing the patient’s vital signs. Le Fort fractures require unstable fracture segment fixation on stable structures [11]. The management goals are form and function restoration.
In Le Fort fractures, the pterygoid process must also be surgically stabilized [12]. The pterygoid plate is a structure that is not easily accessible under general conditions due to its positional characteristics. The lateral pterygoid muscle is attached to the posterior surface of the pterygoid plates. Healing of the intentionally fractured plate could have several problems due to these anatomical features. Gradual displacement or movement of a fractured piece of the pterygoid plate can occur due to the action of the lateral pterygoid muscle. Furthermore, considering the presence of the vessels in proximity to the pterygoid process, particularly the descending palatine artery in the anterior part and the pterygoid venous plexus in the posterior part, is necessary. The blood vessels wrapped around the bone must be properly detached and managed due to the high risk of massive bleeding if the plate fracture is inappropriately managed; therefore, correct osteotomy direction and proper pterygoid plate separation are required [12].
Our case is therefore a rare example of an isolated pterygoid plate fracture without associated Le Fort or mandibular fractures. Our patient presented only the fracture of the medial wall of the ipsilateral maxillary sinus.
Thin-slice high-resolution CT imaging is the gold standard for diagnosing facial fractures and making decisions for treatment. The axial and reformatted CT images also show the degree of bone fragment displacement and contiguous soft tissue alterations [13].
Isolated pterygoid plate fractures are not treated surgically. For patients with isolated pterygoid plate fracture, a soft diet is recommended until the fracture heals to avoid jaw pain [14].
CONCLUSION
Approximately, one-third of pterygoid plate fractures are unrelated to Le Fort fractures but are present alone or associated with other facial skeleton fractures. The radiologist’s knowledge of these other types of fracture is important for making a differential diagnosis in patients with facial trauma. CT imaging is essential to diagnose fractures, describe the fragment location in displaced fractures, and guide the surgeon in choosing the treatment.
ADDITIONAL INFORMATION
Funding source. This publication was not supported by any external sources of funding.
Competing interests. Authors declare no explicit and potential conflicts of interests associated with the publication of this article.
Authors’ contribution. All authors made a substantial contribution to the conception of the work, acquisition, analysis, interpretation of data for the work, drafting and revising the work, final approval of the version to be published and agree to be accountable for all aspects of the work.
Consent for publication. Written consent was obtained from the patient for publication of relevant medical information and all of accompanying images within the manuscript.
Sobre autores
Rosario Francesco Balzano
Radiology Unit, Barletta University Campus UNIFG, “Dimiccoli” Hospital
Email: ro.balzano@gmail.com
Itália, Foggia
Valentina Testini
Department of Clinical and Experimental Medicine, Foggia University School of Medicine
Email: testinivalentina@gmail.com
Itália, Foggia
Aldo Cammarota
Radiation Oncology Unit, IRCCS CROB, Rionero in Vulture
Email: aldo.cammarota@crob.it
Itália, Potenza
Giuseppe Guglielmi
Radiology Unit, Barletta University Campus UNIFG, “Dimiccoli” Hospital; Department of Clinical and Experimental Medicine, Foggia University School of Medicine; Radiology Unit, Hospital “Casa Sollievo Della Sofferenza”, San Giovanni Rotondo
Autor responsável pela correspondência
Email: giuseppe.guglielmi@unifg.it
ORCID ID: 0000-0002-4325-8330
Medical Doctor, Full Professor of Radiology, Department of Clinical and Experimental Medicine.
Itália, Foggia; Foggia; FoggiaBibliografia
- Boffano P, Roccia F, Zavattero E, et al. European Maxillofacial Trauma (EURMAT) project: a multicentre and prospective study. J Craniomaxillofac Surg. 2015;43(1):62–70. doi: 10.1016/j.jcms.2014.10.011
- Winegar BA, Murillo H, Tantiwongkosi B. Spectrum of critical imaging findings in complex facial skeletal trauma. Radiographics. 2013;33(1):3–19. doi: 10.1148/rg.331125080
- Le Fort R: Etude experimentale sur les fractures de la machoire superieure. Rev Chir. 1901;23:208–507.
- Patel BC, Wright T, Waseem M. Le Fort Fractures. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
- Choi JW, Kim MJ. Treatment of panfacial fractures and three-dimensional outcome analysis: the occlusion first approach. J Craniofac Surg. 2019;30(4):1255–1258. doi: 10.1097/SCS.0000000000005528
- Surya M, Soni P, Bharti R, Jamwal I. Isolated fracture of lateral pterygoid plate by penetrating foreign body ― a rarity indeed. Pol J Radiol. 2017;82:137–140. doi: 10.12659/PJR.900407
- Garg RK, Alsheik NH, Afifi AM, Gentry LR. Pterygoid plate fractures: not limited to Le Fort Fractures. J Craniofac Surg. 2015;26(6):1823–1825. doi: 10.1097/SCS.0000000000001901
- Truong AQ, O’Brien DC, Strong EB, Dublin A. Lateral pterygoid plate fractures associated with mandible fractures. JAMA Facial Plast Surg. 2014;16(6):437–439. doi: 10.1001/jamafacial.2014.645
- Unger JM, Gentry LR, Grossman JE. Sphenoid fractures: prevalence, sites, and significance. Radiology. 1990;175(1):175–180. doi: 10.1148/radiology.175.1.2315477
- Murray GM, Phanachet I, Uchida S, et al. The human lateral pterygoidmuscle: a review of some experimental aspects and possible clinical relevance. Aust Dent J. 2004;49(1):2–8. doi: 10.1111/j.1834-7819.2004.tb00042.x
- Phang SY, Whitehouse K, Lee L, et al. Management of CSF leak in base of skull fractures in adults. Br J Neurosurg. 2016;30(6):596–604. doi: 10.1080/02688697.2016.1229746
- Choi NR, Shin SH, Kim SS, et al. Healing pattern of intentional pterygoid plate fracture after posterior movement of maxilla through Le Fort I osteotomy. J Craniomaxillofac Surg. 2018;46(10):1828–1833. doi: 10.1016/j.jcms.2018.08.003
- Kaeppler G, Cornelius CP, Ehrenfeld M, Mast G. Diagnostic efficacy of cone-beam computed tomography for mandibular fractures. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116 (l):98–104. doi: 10.1016/j.oooo.2013.04.004
- De Oliveira DM, Vasconcellos RJ, Filho JR, Cypriano RV. Fracture of the coronoid and pterygoid processes by firearms: case report. Braz Dent J. 2007;18(2):168–170. doi: 10.1590/s0103-64402007000200016
Arquivos suplementares

