







Autoimmune hypophysitis: a case of follow-up during the COVID-19 pandemic period
- Authors: Surovcev E.N.1,2, Zelter P.M.1,3, Kapishnikov A.V.1, Pyshkina Y.S.1
-
Affiliations:
- Samara State Medical University
- Diagnostic and treatment center of International institution for biological systems named after Sergey Berezin
- Meir Hospital
- Issue: Vol 6, No 1 (2025)
- Pages: 178-186
- Section: Case reports
- Submitted: 23.07.2024
- Accepted: 16.10.2024
- Published: 25.03.2025
- URL: https://jdigitaldiagnostics.com/DD/article/view/634533
- DOI: https://doi.org/10.17816/DD634533
- ID: 634533

Cite item
Full Text

Abstract
Hypophysitis is a rare inflammatory disorder that affects the pituitary gland and infundibulum, stems from autoimmune, infiltrative, infectious, or unknown causes. Its clinical diagnosis can be challenging because several pituitary lesions, including adenomas and metastases, may clinically present with similar characteristics. Magnetic resonance imaging is crucial for diagnosing suspected cases of hypophysitis and categorizing them as adenohypophysitis (anterior pituitary gland involvement) or infundibulo-neurohypophysitis (pituitary stalk and posterior pituitary involvement). Hypophysitis can be categorized as primary (autoimmune) or secondary due to local lesions (e.g., granulomas, cysts, adenomas) or systemic diseases (e.g., sarcoidosis, Wegener’s granulomatosis). Different factors may have impact on clinical course of hypophysitis. Among them background treatment. These cases have not been sufficiently studied and are practically not presented in publications.
A 37-year-old female with a history of hyperprolactinemia was being treated symptomatically with cabergoline. At first magnetic resonance imaging heterogeneity of the hypophysis was revealed. In September 2021 the follow-up magnetic resonance imaging revealed an increase in the size and heterogeneity of the pituitary gland. In December 2021, the patient developed severe COVID-19-associated pneumonia and was treated with corticosteroids and oxygen support. In May 2022 magnetic resonance imaging revealed a marked increase in the size and heterogeneity of the pituitary gland. Significant clinical and radiological improvement were stated after adding prednisone (10 mg in the morning and 5 mg in the evening) to her treatment.
The patient was followed-up during the COVID-19 pandemic. The management and imaging studies of such patients may be tricky due to the effects related to COVID-19 and its treatment.
During monitoring of hypophysitis, physicians should consider the impact of COVID-19 treatment, particularly corticosteroid therapy, when evaluating the radiological changes.
Full Text
АКТУАЛЬНОСТЬ
Гипофизит — редкое воспалительное заболевание, характеризующееся поражением гипофиза и его ножки. Данная патология может возникать в результате новообразований и инфильтрации гипофиза, действия аутоиммунных факторов, перенесённого инфекционного заболевания или под влиянием других неустановленных причин. Распространённость гипофизита составляет приблизительно 1 случай на 9 млн человек [1]. Его клиническая диагностика вызывает трудности, поскольку некоторые новообразования гипофиза, в том числе широко распространённые аденомы и редко встречающиеся метастазы, могут иметь сходные клинические характеристики [2].
Магнитно-резонансная томография (МРТ) — основной метод диагностики гипофизита, а также дифференциальной диагностики аденогипофизита (поражение передней доли гипофиза) и инфундибулонейрогипофизита (поражение ножки и задней доля гипофиза). Различают два вида гипофизита: первичный (аутоиммунный) и вторичный, возникающий из локализованных очагов (например, гранулём, кист или аденом) или в результате системных заболеваний (например, саркоидоза, гранулематоза с полиангиитом) [3, 4].
Диагноз аутоиммунного гипофизита (АГ) ставят только после исключения его вторичных причин. При обследовании всех пациентов в соответствии с диагностическими критериями следует исключить гранулематозный васкулит, саркоидоз и гистиоцитоз из клеток Лангерганса [5].
АГ имеет следующие радиологические признаки:
- увеличение гипофиза (симметричное или асимметричное);
- гомо- или гетерогенный характер накопления контрастного вещества;
- утолщение ножки гипофиза;
- супраселлярное и/или параселлярное разрастание аденомы гипофиза;
- отсутствие типичного гиперинтенсивного сигнала в задней доле гипофиза на T1-взвешенных изображениях;
- возможное наличие «дурального хвоста»;
- гиперинтенсивность сигнала параселлярной области на T2-взвешенных изображениях.
Радиологические признаки могут быть слабо выражены и в некоторых случаях их обнаружение возможно только при сравнении с результатами предыдущих визуализационных исследований [6]. Клиническое течение гипофизита зависит от разных факторов, один из которых — базисная терапия. В отечественной и зарубежной литературе описаны клинические случаи гипофизита [3, 7].
Мы решили продемонстрировать случай АГ у пациентки во время пандемии COVID-19 с целью выявления его особенностей в соответствии с данными МРТ и клинического течения.
ОПИСАНИЕ СЛУЧАЯ
Анамнез
Женщина в возрасте 37 лет с гиперпролактинемией в анамнезе. По результатам исследования от декабря 2019 г. содержание пролактина составило 2144 мМЕ/л (референсные значения: 109–557 мМЕ/л). В мае 2020 г. пациентка проходила МРТ головного мозга по направлению лечащего врача, на момент обследования не предъявляла каких-либо жалоб и получала симптоматическое лечение агонистом дофаминовых рецепторов каберголином в дозе 0,25 мг два раза в сутки для подавления выработки пролактина.
Результаты лабораторного и инструментального исследований
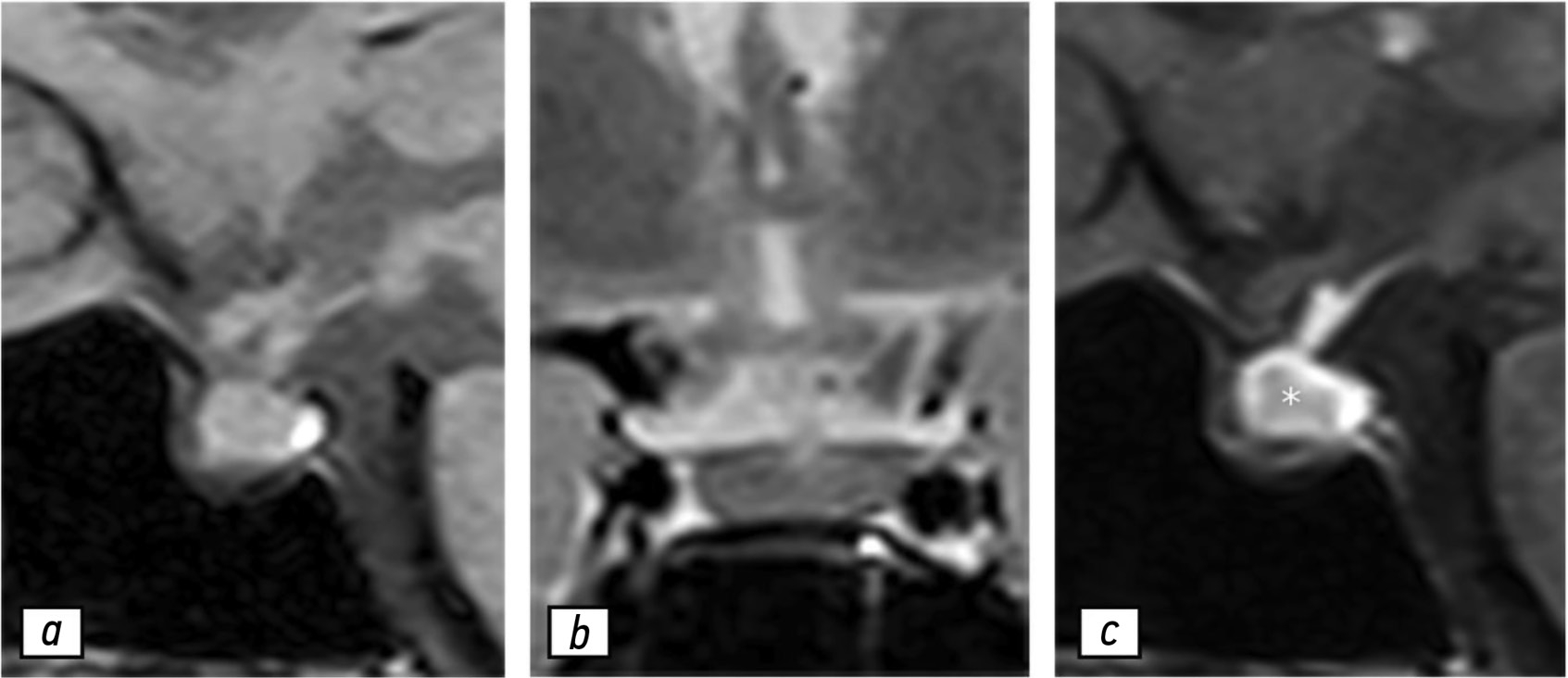
Согласно данным МРТ гипофиза с контрастированием (рис. 1), гипофиз имел слегка гетерогенную структуру и нормальные размеры:
- в сагиттальной плоскости — 1,3 см;
- в вертикальной плоскости — 1 см;
- во фронтальной плоскости — 2 см.

Рис. 1. Результаты магнитно-резонансной томографии гипофиза, 02.05.2020: a — T1-взвешенное изображение в сагиттальной проекции; b — T2-взвешенное изображение в коронарной проекции; с — T1-взвешенное изображение в сагиттальной проекции с контрастированием. Гипофиз (звёздочка) не увеличен и имеет слегка гетерогенную структуру.
Отмечено незначительное отклонение ножки гипофиза влево. После введения гадолиний-содержащего контрастного вещества в центре вещества гипофиза обнаружено незначительное неравномерное усиление магнитно-резонансного сигнала. Несмотря на то что клиникорадиологическая картина не демонстрировала наличие гипофизита, рекомендовано проведение контрольной МРТ по причине гетерогенности структуры гипофиза.
Результаты контрольной МРТ, выполненной в июле 2021 г., продемонстрировали увеличение гипофиза и усиление гетерогенности его структуры, что можно рассматривать как первые признаки гипофизита (рис. 2). В сентябре 2021 г. у пациентки не обнаружено каких-либо специфических симптомов, кроме головной боли. При проведении лабораторных исследований выявлено значимое снижение концентрации пролактина — 96,6 мМЕ/л.

Рис. 2. Результаты магнитно-резонансной томографии гипофиза, 09.07.2021: a — T1-взвешенное изображение в сагиттальной проекции; b — T2-взвешенное изображение в коронарной проекции; с — T1-взвешенное изображение в сагиттальной проекции с контрастированием. Отмечено умеренное увеличение гипофиза, усиление сигнала в его веществе (звёздочка) на T2-взвешенных изображениях (b), а также гетерогенное накопление контрастного вещества в центральной области гипофиза.
Дополнение к анамнезу
В декабре 2021 г. у пациентки на фоне COVID-19 диагностировали тяжёлую пневмонию с поражением около 75% паренхимы лёгких. Ей назначили лечение в виде глюкокортикостероидов и кислородной терапии. Через месяц после выписки из стационара, в январе 2022 г., пациентка обратилась к эндокринологу с жалобами на тошноту, сильную слабость, головокружение и снижение артериального давления. В результате обследования выявлены гипопролактинемия, признаки гипотиреоза и недостаточность коры надпочечников.
Дифференциальная диагностика
В связи с увеличением гипофиза дифференциальная диагностика проведена со следующими заболеваниями:
- аденома гипофиза — чаще гиповаскулярная;
- менингиома — наличие характерных признаков распространения по твёрдой мозговой оболочке;
- метастазы — отсутствие данных о первичной опухоли;
- некоторые формы гипофизита — отсутствие возможностей дифференцировать при визуализации [6].
Последующее наблюдение и исход
С учётом изменения гормонального статуса пациентки и ухудшения её состояния рекомендовано выполнение МРТ гипофиза (рис. 3). При её проведении не выявлено каких-либо значимых изменений его размера или структуры. Тем не менее отмечено резкое утолщение ножки гипофиза и хиазмы, а также усиление гетерогенности структуры. С целью коррекции гипотиреоза пациентке назначен левотироксин натрия — 25 мкг в сутки. Лечение каберголином продолжено с учётом ранее рекомендованной дозы. На фоне лечения пациентка отмечала усиление тошноты, головокружения и общую слабость.

Рис. 3. Результаты магнитно-резонансной томографии гипофиза, 04.02.2022: a — T1-взвешенное изображение в сагиттальной проекции; b — T2-взвешенное изображение в коронарной проекции; с — T1-взвешенное изображение в сагиттальной проекции с контрастированием. Отмечено прогрессирование очага, утолщение хиазмы (стрелки) и ножки гипофиза. Увеличение гипофиза и неоднородности его структуры наблюдали без выраженной динамики по сравнению с данными за 09.07.2021.
В мае 2022 г. у пациентки возник эпизод тяжёлой артериальной гипотензии (80/50 мм рт. ст.). С диагнозом недостаточности коры надпочечников пациентку госпитализировали в отделение эндокринологии. Результаты исследования содержания гормонов указывали на наличие признаков гипотиреоза и недостаточности коры надпочечников. Кроме того, при проведении МРТ головного мозга отмечено выраженное увеличение гипофиза и усиление гетерогенности его структуры (рис. 4).

Рис. 4. Результаты магнитно-резонансной томографии гипофиза, 02.05.2022: a — T1-взвешенное изображение в сагиттальной проекции; b — T2-взвешенное изображение в коронарной проекции; с — T1-взвешенное изображение в сагиттальной проекции с контрастированием. Отмечено резкое увеличение гипофиза, в основном за счёт супраселлярного компонента, структура неоднородна, контуры неровные. Хиазма сдавлена. Выявлено выраженное неравномерное утолщение слизистой оболочки клиновидной пазухи (звёздочки) в виде усиления интенсивности сигнала на T2-взвешенном изображении (b).
На этом этапе пациентка получала преднизон (утром и вечером — 10 и 5 мг соответственно) и каберголин (0,25 мг два раза в неделю). На фоне лечения состояние пациентки улучшилось. При проведении контрольной МРТ 03.10.2022 выявлено выраженное уменьшение гипофиза и снижение гетерогенности его структуры (рис. 5).

Рис. 5. Результаты магнитно-резонансной томографии гипофиза, 03.10.2022: a — T1-взвешенное изображение в сагиттальной проекции; b — T2-взвешенное изображение в коронарной проекции; с — T1-взвешенное изображение в сагиттальной проекции с контрастированием. Гипофиз не увеличен, в центральных отделах наблюдается гетерогенное накопление контрастного вещества. Хиазма утолщена и имеет умеренно гетерогенную структуру. Отмечены положительные изменения по сравнению с предыдущими данными магнитно-резонансной томографии.
ОБСУЖДЕНИЕ
АГ — редкое заболевание, наличие которого следует подозревать у пациентов с нарушениями функций гипофиза или со стороны нервной системы и органов зрения (например, головной болью и дефектами поля зрения), которые сопровождаются характерными неврологическими и радиологическими признаками [8]. АГ требует проведение иммуносупрессивной терапии, в частности глюкокортикостероидами. Тем не менее следует проявлять осторожность при их назначении пациентам, уже получающим данный препарат в связи с другими заболеваниями, например ревматической патологией или инфекциями [9]. Клинические и магнитно-резонансные признаки гипофизита представлены в табл. 1 [1, 10].
Таблица 1. Клинические характеристики и магнитно-резонансные признаки гипофизита
Виды гипофизита | Клинические характеристики | Магнитно-резонансные признаки |
Первичный: · лимфоцитарный; · гранулематозный; · ксантоматозный; · некротизирующий; · IgG4-ассоциированный (плазмоцитарный); · смешанный. Вторичный: · иммуномодулирующая терапия как провоцирующий фактор; · появление образований в области турецкого седла и хиазмы. | Клинические проявления неспецифические: · головная боль; · нарушения зрения — в результате сдавления хиазмы; · признаки недостаточности функции гипофиза и (или) несахарный диабет. Лимфоцитарный и ксантоматозный — чаще встречают у женщин. Гранулематозный — в равной степени встречают как у мужчин, так и у женщин. IgG4-ассоциированый — при системных заболеваниях, сопровождающихся возникновением очагов воспаления в поджелудочной железе, желчных путях, забрюшинном пространстве, средостении, щитовидной железе, мочеполовых путях, слюнных и слёзных железах, структурах глазницы, лимфатических узлах, аорте, перикарде, лёгких, почках, коже, желудке, предстательной железе, яичниках. Иммуномодулирующая терапия как провоцирующий фактор — применение противоопухолевой иммунотерапии. | · симметричное увеличение гипофиза; · аденогипофиз неоднородный с кистозными компонентами; · интенсивное неоднородное накопление контрастного вещества после его введения; · возможное наличие «дурального хвоста»; · разрастание в супраселлярную область. Лимфоцитарный и гранулематозный: · утолщение и неоднородность структуры ножки гипофиза; · гиперинтенсивность хиазмы и зрительных путей в T2-режиме. Ксантоматозный: · поражение аденогипофиза без изменений в ножке. Образования в области турецкого седла и хиазмы: · чаще всего герминогенные опухоли или кисты кармана Ратке; · реже краниофарингиомы или аденомы. |
Особенность случая АГ, который мы рассматриваем, состоит в динамическом наблюдении с помощью визуализационного метода — МРТ. С момента первого подозрения на наличие гипофизита до назначения специфического лечения прошёл 21 месяц. За это время изменения, обнаруженные с помощью МРТ, указывали на постепенное прогрессирование патологического процесса с последующим появлением заметных радиологических признаков и клинических проявлений. На фоне терапии глюкокортикостероидами наблюдали исчезновение клинических симптомов и изменений гипофиза, обнаруженных при проведении МРТ [7, 11].
У пациентки выявлена тенденция к усилению, а в дальнейшем к ослаблению клинических и радиологических симптомов (рис. 6), что сопровождалось соответствующими изменениями содержания гормонов в сыворотке крови. На фоне применения глюкокортикостероидов её состояние улучшилось. Тем не менее после выписки из инфекционного стационара терапию глюкокортикостероидами, назначенную по поводу COVID-19, прекратили, что привело к резкому ухудшению состояния. Таким образом, лечение COVID-19 может влиять на течение других заболеваний, в частности АГ.

Рис. 6. T1-взвешенные изображения гипофиза в коронарной проекции с контрастированием: a — нормальные размеры и слегка гетерогенная структура; b, c — постепенное увеличение гипофиза в течение 21 месяца; d — выраженное увеличение гипофиза в течение трёх месяцев, наличие неконтрастной области, вероятно, вследствие некроза (звёздочка); e — гипофиз не увеличен, отмечена положительная динамика.
ЗАКЛЮЧЕНИЕ
Рассматриваемый клинический случай даёт возможность продемонстрировать характерные изменения магнитно-резонансных признаков у пациентки с АГ — усиление радиологических паттернов с одновременным прогрессированием клинических симптомов в результате несвоевременного лечения. После назначения глюкокортикостероидов наблюдали быстрое купирование симптомов, что свидетельствует об их важной роли в лечении данного заболевания. Даже после окончании пандемии клиницистам следует учитывать влияние COVID-19 на течение других заболеваний, в частности АГ.
ДОПОЛНИТЕЛЬНАЯ ИНФОРМАЦИЯ
Источник финансирования. Авторы заявляют об отсутствии внешнего финансирования при проведении работы.
Раскрытие интересов. Авторы заявляют об отсутствии отношений, деятельности и интересов (личных, профессиональных или финансовых), связанных с третьими лицами (коммерческими, некоммерческими, частными), интересы которых могут быть затронуты содержанием статьи, а также иных отношений, деятельности и интересов за последние три года, о которых необходимо сообщить.
Вклад авторов. Е.Н. Суровцев — обследование пациентки, сбор и анализ литературных данных, написание текста рукописи; П.М. Зельтер, Ю.С. Пышкина — сбор и анализ литературных данных, написание и редактирование рукописи; А.В. Капишников — анализ литературных данных, редактирование рукописи. Все авторы одобрили рукопись (версию для публикации), а также согласились нести ответственность за все аспекты работы и гарантировали, что вопросы, связанные с точностью или добросовестностью любой части работы, будут должным образом рассмотрены и решены.
Информированное согласие на публикацию. Авторы получили письменное согласие пациентки на публикацию медицинских данных и изображений в обезличенной форме в журнале Digital Diagnostics.
ADDITIONAL INFORMATION
Funding source. This article was not supported by any external sources of funding.
Disclosure of interests. The authors declare that they have no relationships, activities or interests (personal, professional or financial) with third parties (commercial, non-commercial, private) whose interests may be affected by the content of the article, as well as no other relationships, activities or interests over the past three years that must be reported.
Authors’ contribution. E.N. Surovcev: examination of the patient, collection and analysis of literature data, writing the text of the manuscript; P.M. Zelter, Yu.S. Pyshkina: collection and analysis of literature data, writing and editing the text of the manuscript; A.V. Kapishnikov: analysis of literature data, editing the text of the manuscript. Thereby, all authors provided approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Consent for publication. Written consent was obtained from the patient for publication of relevant medical information and all of accompanying images within the manuscript in Digital Diagnostics journal.
About the authors
Evgeniy N. Surovcev
Samara State Medical University; Diagnostic and treatment center of International institution for biological systems named after Sergey Berezin
Email: evgeniisurovcev@mail.ru
ORCID iD: 0000-0002-8236-833X
SPIN-code: 5252-5661
MD, Cand. Sci. (Medicine)
Russian Federation, Samara; TolyattiPavel M. Zelter
Samara State Medical University; Meir Hospital
Email: pzelter@mail.ru
ORCID iD: 0000-0003-1346-5942
SPIN-code: 3678-3932
MD, Cand. Sci. (Medicine)
Russian Federation, Samara; Kfar-Sava, IsraelAleksandr V. Kapishnikov
Samara State Medical University
Email: a.kapishnikov@gmail.com
ORCID iD: 0000-0002-6858-372X
SPIN-code: 6213-7455
MD, Dr. Sci. (Medicine), Professor
Russian Federation, SamaraYuliya S. Pyshkina
Samara State Medical University
Author for correspondence.
Email: yu.pyshkina@yandex.ru
ORCID iD: 0000-0002-7241-6828
SPIN-code: 4225-1020
MD, Cand. Sci. (Medicine), Assistant Professor
Russian Federation, SamaraReferences
- Uccella S, Dottermusch M, Erickson L, et al. Inflammatory and infectious disorders in endocrine pathology. Endocr Pathol. 2023;34(4):406–436. doi: 10.1007/s12022-023-09771-3 EDN: XJTAXG
- Caturegli P. Autoimmune hypophysitis: an underestimated disease in search of its autoantigen(s). J Clin Endocrinol Metab. 2007;92(6):2038–2040. doi: 10.1210/jc.2007-0808
- Vorontsov AV, Babaeva DM, Vladimirova VP, et al. Clinical and radiological diagnosis of hypophysitis: a review of literature and own data. Problems of Endocrinology. 2022;68(2):16–33. doi: 10.14341/probl12777 EDN: LPMHZL
- Wright K, Kim H, Hill T, et al. Preoperative differentiation of hypophysitis and pituitary adenomas using a novel clinicoradiologic scoring system. Pituitary. 2022;25(4):602–614. doi: 10.1007/s11102-022-01232-0 EDN: XQPLFK
- Tsukamoto T, Miki Y. Imaging of pituitary tumors: an update with the 5th WHO classifications-part 2. Neoplasms other than PitNET and tumor-mimicking lesions. Jpn J Radiol. 2023;41(8):808–829. doi: 10.1007/s11604-023-01407-0 EDN: CGTFFL
- Tartaglione T, Chiloiro S, Laino ME, et al. Neuro-radiological features can predict hypopituitarism in primary autoimmune hypophysitis. Pituitary. 2018;21(4):414–424. doi: 10.1007/s11102-018-0892-4 EDN: GTNYNU
- Karrou M, Benyakhlef S, Alla A, et al. Clinical presentation and management of hypophysitis: an observational study of case series. Surg Neurol Int. 2021;12:304. doi: 10.25259/sni_454_2021 EDN: ZYMRCD
- Caturegli P, Lupi I, Landek-Salgado M, et al. Pituitary autoimmunity: 30 years later. Autoimmun Rev. 2008;7(8):631–637. doi: 10.1016/j.autrev.2008.04.016 EDN: MEPFHV
- Ravindran R, Carter JL, Kumar A, et al. Pre-test cortisol levels in predicting short synacthen test outcome: a retrospective analysis. Clin Med Insights Endocrinol Diabetes. 2022;15:11795514221093316. doi: 10.1177/11795514221093316 EDN: APQAJS
- Langlois F, Varlamov EV, Fleseriu M. Hypophysitis, the growing spectrum of a rare pituitary disease. J Clin Endocrinol Metab. 2022;107(1);10–28. doi: 10.1210/clinem/dgab672 EDN: YLEGQC
- Al Argan R, Ramadhan A, Agnihotram RV, et al. Baseline MRI findings as predictors of hypopituitarism in patients with non-functioning pituitary adenomas. Endocr Connect. 2021;10(11):1445–1454. doi: 10.1530/ec-21-0386 EDN: SQCXNL
Supplementary files

