

")






年轻患者睾丸破裂以及对比增强超声检查的诊断价值
- 作者: Eusebi L.1, Paparella M.T.2, Marconi A.3, Guglielmi G.2,4
-
隶属关系:
- Radiology Unit, “Carlo Urbani” Hospital
- Department of Clinical and Experimental Medicine, Foggia University School of Medicine
- Department of Urology, “Carlo Urbani” Hospital
- Radiology Unit, Barletta University Campus UNIFG, “Dimiccoli” Hospital
- 期: 卷 3, 编号 1 (2022)
- 页面: 78-85
- 栏目: 临床病例及临床病例的系列
- ##submission.dateSubmitted##: 13.12.2021
- ##submission.dateAccepted##: 02.03.2022
- ##submission.datePublished##: 24.04.2022
- URL: https://jdigitaldiagnostics.com/DD/article/view/90277
- DOI: https://doi.org/10.17816/DD90277
- ID: 90277

如何引用文章

详细
由于阴囊钝性伤发生的睾丸破裂的特点是鞘膜受损,导致细精管挤压。
显现法,尤其是超声,在评估阴囊损伤方面发挥着至关重要的作用,并允许确定患者管理的进一步策略 - 保守治疗或外科手术。标准B模式超声和彩超是评估睾丸损伤的主要显现法,但对睾丸损伤的程度意义不大。 外科医生最重要的信息是鞘膜的完整性或破裂以及睾丸重要组织的损伤程度。由于水肿破坏了血管血流,导致睾丸的血管形成过多,仅从标准的超声检查的数据很难判断后者。如果彩色多普勒绘图的结果不确定,则必须使用其他现代成像方式,如造影剂增强超声,以确定受伤睾丸的生存能力。
本文描述了一名15岁足球运动员睾丸钝性伤的临床病例。
全文:
绪论
青年男性阴囊创伤占全部创伤相关性损伤的1%以下[1]。约1.5%的阴囊钝性创伤病例可见睾丸破裂[2]。过去十年内报告的病例不到60例[3]。
睾丸在阴囊内的活动度受白膜、被覆皮肤的松弛度和提睾肌的收缩反射的保护。白膜以其巨大的抗张强度,对保护睾丸起着至关重要的作用;白膜可以承受高达50kg的力而不破裂[2]。生殖器皮肤松弛可保护下层脏器免受钝性创伤,使其从接触点滑走;然而,如果生殖器皮肤持续被困在旋转机器中,过度的皮肤松弛可导致严重损伤,导致一侧或双侧睾丸撕脱和破裂[4]。体育活动占所有睾丸损伤病例的50%以上,机动车碰撞是阴囊创伤的另一原因[5,6]。
钝性损伤是由于接触固体物(例如,腹股沟踢击或棒球或曲棍球棒撞击)期间转移的高能量导致的非侵入性损伤。主要损伤机制是睾丸在耻骨联合或大腿间的挤压。在大多数男性中,右侧睾丸损伤更为频繁,因为右侧睾丸的解剖位置略高于左侧睾丸[7]。阴囊创伤可引起睾丸实质出血和梗死,进而导致坏死。在严重损伤中,可发生白膜破坏并伴有实质突出。提示需进行紧急手术以挽救睾丸[8]。此外,早期修复至关重要,因为破裂可能损伤血液睾丸屏障,随后形成抗精子细胞的抗体,导致不育[9]。
本病例研究描述了1例15岁足球运动员睾丸钝性创伤的评估和治疗。
病例描述
一名15岁健康男性青少年在足球比赛中被踢中腹股沟,击中阴囊。患者立即出现重度疼痛。数小时后,虽然症状有所改善,但因左侧阴囊持续肿胀、发紫,来我院急诊科就诊。未报告任何其他损伤。
泌尿生殖系统检查发现,左侧阴囊比右侧大约2倍,有严重瘀斑。由于疼痛和肿胀,左侧睾丸难以触诊,而右侧睾丸大小正常,未见任何明显异常。左侧提睾反射未引出。
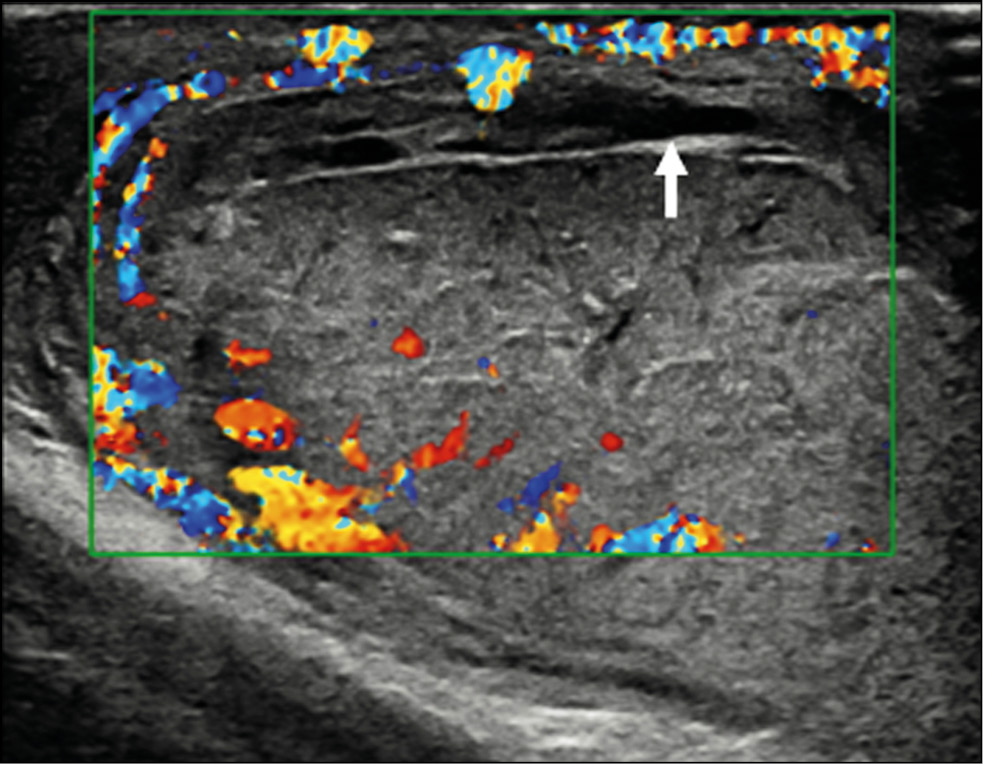
阴囊超声检查(US)示阴囊中度水肿、积血,伴白膜不连续,特征为白膜轮廓异常(图1)。彩色多普勒超声(CDUS)提示上极血管缺失,挤入睾丸破裂部分约2.5cm(图2)。但无扭伤或梗死迹象。申请泌尿外科会诊,行造影剂增强超声(CEUS),确诊为睾丸破裂,确定了重要实质的量(图3)。

图1 B超检查影像。(a)代表破裂指数的白膜中断伴回声物质突出(箭头);(b)睾丸内挫伤引起的中等量积血( 箭头)和睾丸实质不均表现。

图2彩色多普勒超声影像显示睾丸形态不规则,断裂点存在无血管区(箭头)。

图3 造影剂增强超声可确定重要实质的范围,帮助术前决策过程,允许重要睾丸组织恢复,避免睾丸切除。
根据超声结果,患者住院接受左半阴囊紧急检查。术中抽出大量积血,仔细检查睾丸发现白膜有病变。行白膜直接缝合(图4)。患者顺利康复,4天后出院。

图4术中影像:(a)证实白膜破裂;(b)白膜直接缝合。
讨论
阴囊病变的鉴别诊断包括附睾炎、睾丸炎、腹股沟嵌顿疝、睾丸梗死、睾丸骨折或破裂、睾丸扭转、阑尾扭转、睾丸脱位、鞘膜积液或积血等[10]。根据欧洲泌尿外科学会指南,CDUS是研究阴囊创伤病理学的一线成像模式[11]。因此,评价血管灌注和睾丸完整性,对区分睾丸破裂和其他病变具有重要意义。利用现代超声设备,目前诊断睾丸破裂的敏感性和特异性可达95%-100%[12]。正常白膜表现为围绕睾丸实质的纤细低回声线。在存在积血的情况下可能很难鉴别。除检查白膜的完整性外,还应检查睾丸轮廓的规整性。本质上来讲,当睾丸破裂时,睾丸会因为实质挤压而失去正常的椭圆形形态[13]。因此,睾丸形态的不规则是白膜破裂的一个间接征象。其他超声表现包括不均匀回声、鞘膜破裂、穿过睾丸的骨折线、血流减少或缺失、阴囊增厚和积血形成。CDUS在创伤后阴囊评估中不可或缺 [14] ,因为白膜破裂总是伴有血管膜(由鞘膜 动脉组成)破裂,进而导致下层实质的血管信号丢失。这一点极其重要,因为它有助于确定睾丸实质的活力[15]。然而,CDUS在急性病例中可能有歧义,因为CDUS可能无法检测低血流状态,尤其是在儿科患者中[16],并且认为它在发现缺血方面不太可靠[17],可能导致适当手术治疗的延迟。
在传统超声诊断存疑情况下,可提议进行CEUS。CEUS对显示受损睾丸的实质血管分布及其变化的敏感性高[18]。欧洲医学和生物学超声学会联合会的官方指南描述了CEUS在许多领域的实用性[19]。通常使用4.8 mL SonoVue™(Bracco Spa,Milan)。CEUS检查的造影剂无肾脏毒性,磷脂外壳可经肝脏代谢,六氟化硫气体成分经肺呼出。该技术可在肾衰竭患者中应用,无需提供既往实验室检查。此外,超声造影剂(UCA)产生不良反应的风险低于计算机断层扫描和磁共振成像中常用的造影剂。CEUS还具有价格低廉、快速、便携、可重复、安全可多次注射等特点,且均无辐射暴露[20]。CEUS中的动脉期是检查的最重要工具。睾丸和附睾强化较快,但可因个体而异。动脉首先强化,然后在数秒内整个实质强化。阴囊壁强化常常低于内容物的强化。强化减低的时间各不相同,通常为3分钟。正常睾丸实质均匀,表面回声线即为白膜。在CEUS上,睾丸应均匀强化,条纹图案代表正常睾丸内血管解剖结构内的UCA[20]。CEUS能更清晰地描绘骨折线、白膜中断以及睾丸内和睾丸外血肿[21]。CEUS可以评估存活睾丸的确切范围,为泌尿科医生决定何时部分挽救器官提供好的解决方案[22]。此外,小的睾丸肿瘤在CDUS中可能表现为无血管;因此,梗死的鉴别可能很困难。CEUS可区分血管化和非血管化睾丸局灶性病变,有助于排除恶性肿瘤。最后,欧洲泌尿生殖放射学会阴囊和阴茎成像工作组提供了立场声明,目的是指导成像运用,尤其是多参数超声在阴囊创伤中的运用。
因此,当无法用CDUS进行诊断时,CEUS可用于识别是否存在血流;在常规超声中识别不明确病例的睾丸破裂、骨折线、血肿和缺血性改变;区分无血管和血管化不良的病变,以区分血肿和肿瘤[23]。
结论
阴囊超声是诊断睾丸创伤的一线影像学检查方法。目前,CEUS是研究阴囊创伤病理的一线成像方式。CEUS有可能成为评估急性阴囊创伤不可或缺的工具,提供准确的诊断性成像,帮助提高医生的决策信心。结合超声设备和CEUS提供的实质血管分布信息,在超声检查中使用造影剂可能是迅速解决模棱两可超声结果的最佳方案。这对于是否进行急诊手术的手术决策尤其相关,最重要的是,可了解受累睾丸是否可挽救。
目前睾丸破裂的治疗策略是72小时内实施手术探查修补,最大限度挽救。
Additional information
Funding source. This study was not supported by any external sources of funding.
Competing interest. Authors declare no explicit and potential conflicts of interests associated with the publication of this article.
Authors’ contribution. All authors made a substantial contribution to the conception of the work; acquisition, analysis, and interpretation of data for the work; drafting and revising the work; final approval of the version to be published; and agree to be accountable for all aspects of the work. L. Eusebi and M.T. Paparella contributed equally to the research work related to the topic and manuscript writing; A. Marconi helped in literature research and data acquisition; G. Guglielmi was involved in the critical revision of the manuscript.
Consent for publication. Written consent was obtained from the patient for the publication of relevant medical information and all accompanying images.

作者简介
Laura Eusebi
Radiology Unit, “Carlo Urbani” Hospital
Email: lauraeu@virgilio.it
ORCID iD: 0000-0002-4172-5126
意大利, Jesi
Maria T. Paparella
Department of Clinical and Experimental Medicine, Foggia University School of Medicine
Email: mt.paparella@gmail.com
ORCID iD: 0000-0003-2573-9509
意大利, Foggia
Andrea Marconi
Department of Urology, “Carlo Urbani” Hospital
Email: andreamarconi3@virgilio.it
意大利, Jesi
Giuseppe Guglielmi
Department of Clinical and Experimental Medicine, Foggia University School of Medicine; Radiology Unit, Barletta University Campus UNIFG, “Dimiccoli” Hospital
编辑信件的主要联系方式.
Email: giuseppe.guglielmi@unifg.it
ORCID iD: 0000-0002-4325-8330
Medical Doctor, Full Professor of Radiology, Department of Clinical and Experimental Medicine.
意大利, Foggia; Foggia参考
- Deurdulian C, Mittelstaedt CA, Chong WK, Fielding JR. US of acute scrotal trauma: optimal technique, imaging findings, and management. Radiographics. 2007;27(2):357–369. doi: 10.1148/rg.272065117
- Bhatt S, Dogra VS. Role of US in testicular and scrotal trauma. Radiographics. 2008;28(6):1617–1629. doi: 10.1148/rg.286085507
- Sadjo SA, Destinval C, Lemelle JL, Berte N. Testicular rupture after blunt scrotal trauma in children: a case report and literature review. Trauma Case Rep. 2021;33:100482. doi: 10.1016/j.tcr.2021.100482
- Wessells H, Long L. Penile and genital injuries. Urol Clin North Am. 2006;33(1):117–126. doi: 10.1016/j.ucl.2005.11.003
- Haas CA, Brown SL, Spirnak JP. Penile fracture and testicular rupture. World J Urol. 1999;17(2):101–106. doi: 10.1007/s003450050114
- Munter DW, Faleski EJ. Blunt scrotal trauma: emergency department evaluation and management. Am J Emerg Med. 1989;7(2):227–234. doi: 10.1016/0735-6757(89)90143-5
- Mulhall JP, Gabram SG, Jacobs LM. Emergency management of blunt testicular trauma. Acad Emerg Med. 1995;2(7):639–643. doi: 10.1111/j.1553-2712.1995.tb03604.x
- Huang DY, Pesapane F, Rafailidis V, et al. The role of multiparametric ultrasound in the diagnosis of paediatric scrotal pathology. Br J Radiol. 2020;93(1110):20200063. doi: 10.1259/bjr.20200063
- Wright S, Hoffmann B. Emergency ultrasound of acute scrotal pain. Eur J Emerg Med. 2015;22(1):2–9. doi: 10.1097/MEJ.0000000000000123
- Wang A, Stormont I, Siddiqui MM. A review of imaging modalities used in the diagnosis and management of scrotal trauma. Current Urology Reports. 2017;18(12):98–103. doi: 10.1007/s11934-017-0744-1
- Kitrey ND, Djakovic N, Gonsalves M, et al. EAU guidelines on urological trauma. European Association of Urology; 2016. Available from: https://uroweb.org/individual-guidelines/non-oncology-guidelines/
- Cannis M, Mailhot T, Perera P. Bedside ultrasound in a case of blunt scrotal trauma. West J Emergency Med. 2013;14(2):127–129. doi: 10.5811/westjem.2012.8.12630
- Bhatt S, Ghazale H, Dogra VS. Sonographic evaluation of scrotal and penile trauma. Ultrasound Clin. 2007;2(1):45–56. doi: 10.1016/j.cult.2007.01.003
- Pepe P, Panella P, Pennisi M, Aragona F. Does color Doppler sonography improve the clinical assessment of patients with acute scrotum? Eur J Radiol. 2006;60(1):120–124. doi: 10.1016/j.ejrad.2006.04.016
- Muttarak M, Thinyu S, Lojanapiwat B. Clinics in diagnostic imaging (114). Rupture of the right testis. Singapore Med J. 2007;48(3):264–268.
- Yusuf G, Konstantatou E, Sellars ME, et al. Multiparametric sonography of testicular hematomas: features on grayscale, color Doppler, and contrast-enhanced sonography and strain elastography. J Ultrasound Med. 2015;34:1319–1328. doi: 10.7863/ultra.34.7.1319
- Hedayati V, Sellars ME, Sharma DM, Sidhu PS. Contrast-enhanced ultrasound in testicular trauma: role in directing exploration, debridement and organ salvage. Br J Radiol. 2012;85(1011):e65–e68. doi: 10.1259/bjr/95600238
- Badea R, Lucan C, Suciu M, et al. Contrast enhanced harmonic ultrasonography for the evaluation of acute scrotal pathology. A pictorial essay. Med Ultrason. 2016;18(1):110–115. doi: 10.11152/mu.2013.2066.181.esy
- Sidhu PS, Cantisani V, Dietrich CF, et al. The EFSUMB guidelines and recommendations for the clinical practice of contrast-enhanced ultrasound (CEUS) in non-hepatic applications: update 2017 (short version). Ultraschall Med. 2018;39(2):154–180. doi: 10.1055/s-0044-101254
- Yusuf GT, Rafailidis V, Moore S, et al. The role of contrast-enhanced ultrasound (CEUS) in the evaluation of scrotal trauma: a review. Insights Imaging. 2020;11(1):68. doi: 10.1186/s13244-020-00874-7
- Trinci M, Cirimele V, Ferrari R, et al. Diagnostic value of contrast-enhanced ultrasound (CEUS) and comparison with color Doppler ultrasound and magnetic resonance in a case of scrotal trauma. J Ultrasound. 2020;23(2):189–194. doi: 10.1007/s40477-019-00389-y
- Valentino M, Bertolotto M, Derchi L, et al. Role of contrast enhanced ultrasound in acute scrotal diseases. Eur Radiol. 2011;21(9):1831–1840. doi: 10.1007/s00330-010-2039-5
- Ramanathan S, Bertolotto M, Freeman S, et al. Imaging in scrotal trauma: a European Society of Urogenital Radiology Scrotal and Penile Imaging Working Group (ESUR-SPIWG) position statement. Eur Radiol. 2021;31(7):4918–4928. doi: 10.1007/s00330-020-07631-w
补充文件

