

")






漏斗胸畸形的磁共振成像
- 作者: Muzafarova G.S.1, Vishnyakova M.V.1, Abramenko A.S.1, Kuzmichev V.A.1, Gatsutsyn V.V.1
-
隶属关系:
- Moscow Regional Research and Clinical Institute
- 期: 卷 5, 编号 2 (2024)
- 页面: 167-177
- 栏目: 原创性科研成果
- ##submission.dateSubmitted##: 07.08.2023
- ##submission.dateAccepted##: 22.03.2024
- ##submission.datePublished##: 20.09.2024
- URL: https://jdigitaldiagnostics.com/DD/article/view/568087
- DOI: https://doi.org/10.17816/DD568087
- ID: 568087

如何引用文章

详细
论证。磁共振成像更常用于确认是否存在漏斗胸畸形,并评估该水平的心脏压迫变化。
目的是通过磁共振成像对漏斗胸畸形进行术前评估。
材料和方法。我们对 38 名患者(30 名男性,8 名女性)的胸部器官磁共振成像进行了回顾性评估。平均年龄为 19.9 岁(±9 岁)。
心脏磁共振成像是在 General Electric Optima MR450w GEM 1.5 特斯拉设备上进行的,使用的是 2D-FIESTA-C 脉冲序列,同时进行了伴有左心室和右心室功能评估的心电图同步。获得了对漏斗胸畸形患者进行进一步手术治疗所需的参数:Haller 指数、矫正指数、胸骨旋转角度。
对获得的数据进行统计处理,寻找 Haller 指数、矫正指数、胸骨旋转角度和右心室射血分数之间的相关性。P<0.05的值被认为是统计学意义的边界。
结果。在 92% 的患者中发现了中度和重度漏斗胸畸形。在寻找 Haller指数值与右心室射血分数之间的相关性时,未发现有统计学意义的 Pearson 相关性(吸气射血分数值的相关性为 P=0.777,呼气射血分数值的相关性为 P=0.798)。右心室射血分数的平均值为 46%。在统计分析中,随着 Haller 指数(胸腔器官畸形程度的增加)的增加,矫正指数也在增加(P<0.05)。44.7% 的患者的胸骨旋转角度值需要修改手术干预(超过15°)。
结论。磁共振成像是一种对漏斗胸畸形有高度参考价值的诊断方法:无需放射线照射,还能对病理变化进行详细的术前评估。
数据显示了,Haller 指数与矫正指数值之间存在相关性(P<0.05)。此外,磁共振成像数据显示了,右心室射血分数有所下降。
全文:
论证
漏斗状胸部畸形(pectus excavatum)是一种常见的胸部发育缺陷(发生率为新生儿的 1:300-1000),其临床表现多见于 10-12 岁和青春期[1, 2]。
在 漏斗状胸部畸形中,胸骨和前肋骨呈不同深度和形状的凹陷。据推测,胸部畸形是肋软骨发育异常,过度生长,导致胸骨进行性移位的结果。这种变化在第 IV 至第 VII 肋骨与胸骨相连处最为明显。当胸骨向前方移位时,可诊断为腹侧型改变,即龙骨状畸形;当胸骨向后方移位时,可诊断为背侧型或漏斗状畸形[2]。
除外观缺陷外,漏斗状胸部畸形还会导致纵隔器官和结构移位以及肺组织受压,从而导致心肺功能改变和体力活动减少 [3-6]。
为了评估变形程度以及改变的胸壁与纵隔器官之间的关系,X射线计算机断层扫描由于其广泛的可用性和研究速度而被广泛使用[3]。
磁共振成像(MRI)也用于确认是否存在畸形以及评估可能的心脏压迫[3]。磁共振成像 无辐射负担,可提供与 CT 类似的胸骨和肋骨状况诊断数据。不过,关于 磁共振成像 在评估手术干预计划所需参数方面的信息量,只有少数资料提供了详细数据[4]。
鉴于确定 漏斗状胸部畸形手术治疗适应症的重要性,各种指数被用来评估病变的严重程度:Haller 指数、矫正指数、胸骨旋转角度的测定。
为了确定Haller指数,在扫描的轴向平面上进行测量。胸廓横向尺寸(以肋骨内侧之间的最大距离测量)与胸廓前后尺寸(脊柱前表面与胸骨后板之间的距离)之比被计算出来[7]。
在 漏斗状胸部畸形中,由于胸骨嵴复合体后退,前胸尺寸减小,从而导致 Haller 指数增加[8]。Haller 指数有以下几种值[8]:
- <2.0 - 正常;
- 2,0~3,2 - 轻度 pectus excavatum;
- 3,2~3,5 - 中度 pectus excavatum;
- >3.5 - 重度 pectus excavatum。
手术矫正 漏斗状胸部畸形的指征是 Haller 指数大于 3.25。
矫正指数是钢板放置后胸部变形的预期增加(式中为最大尺寸与可用最小尺寸之差)与内胸最大前后尺寸的比值乘以100。矫正指数最近被用于确定 漏斗状胸部畸形患者的治疗策略[9]。
胸骨旋转角度的研究对 漏斗状胸部畸形患者至关重要,因为确定角度的表达和方向性可以进一步正确规划手术干预的过程[10]。
目的
根据 磁共振成像 数据对 漏斗状胸部畸形进行有针对性的评估。
材料和方法
研究设计
进行了一项单中心回顾性研究,包括对 38 名患者进行心脏和胸部 磁共振成像 评估。
资格标准
研究的纳入标准:
- 对胸腔器官漏斗状畸形患者进行检查;
- 对心脏和胸部器官进行磁共振成像检查;
- 获得知情同意。
排除标准:
- 体内存在电子起搏器和金属元素;
- 存在幽闭恐惧症;
- 患者行为不当。
医疗干预描述
心脏核磁共振成像检查是手术治疗准备检查的一部分;研究是在通用电气Optima MR450W GEM 1.5 TL设备(GE Healthcare,美国)上使用2D-FIESTA-C脉冲序列进行的,使用 2D-FIESTA-C 脉冲序列。与心电图同步的研究方案包括左心室和右心室心肌的功能评估。功能研究采用标准心轴(长两腔和四腔、短两腔)的标准心脏胶片图像序列(balanced gradient echo)。右心室射血分数的计算在吸气和呼气时以半自动模式进行(对获得的值进行手动校正)。
胸骨漏斗状畸形患者进一步手术治疗所需的参数--Haller指数、矫正指数和胸骨旋转角度--也在心功能研究中获得。
伦理审查
心脏 磁共振成像 是应临床专家的要求作为患者术前评估的一部分进行的,因此在对所进行的研究进行回顾性评估时没有进行伦理检查。
统计分析
研究中所需的样本量没有事先计算。对获得的数据进行统计处理,计算测量参数的平均值和标准偏差。采用 Shapiro-Wilk 标准评估定量指标的分布是否符合正态分布。定量特征的相关性采用 Pearson 和 Spearman 相关性标准进行评估。给出了相关系数值、95%置信区间的界限和达到的p值。评估了双侧显著性水平。p 值小于 0.05 被视为统计学意义的边界。分析在 GraphPad Prism 9(美国 GraphPad 软件公司)中进行。
研究结果
研究对象(参与者)
作为回顾性研究的一部分,对 38 名患者(30 名男性,8 名女性)的心脏和胸部 磁共振成像 数据进行了分析。平均年龄为 19.9 岁(±9 岁)。
HALLER 指数
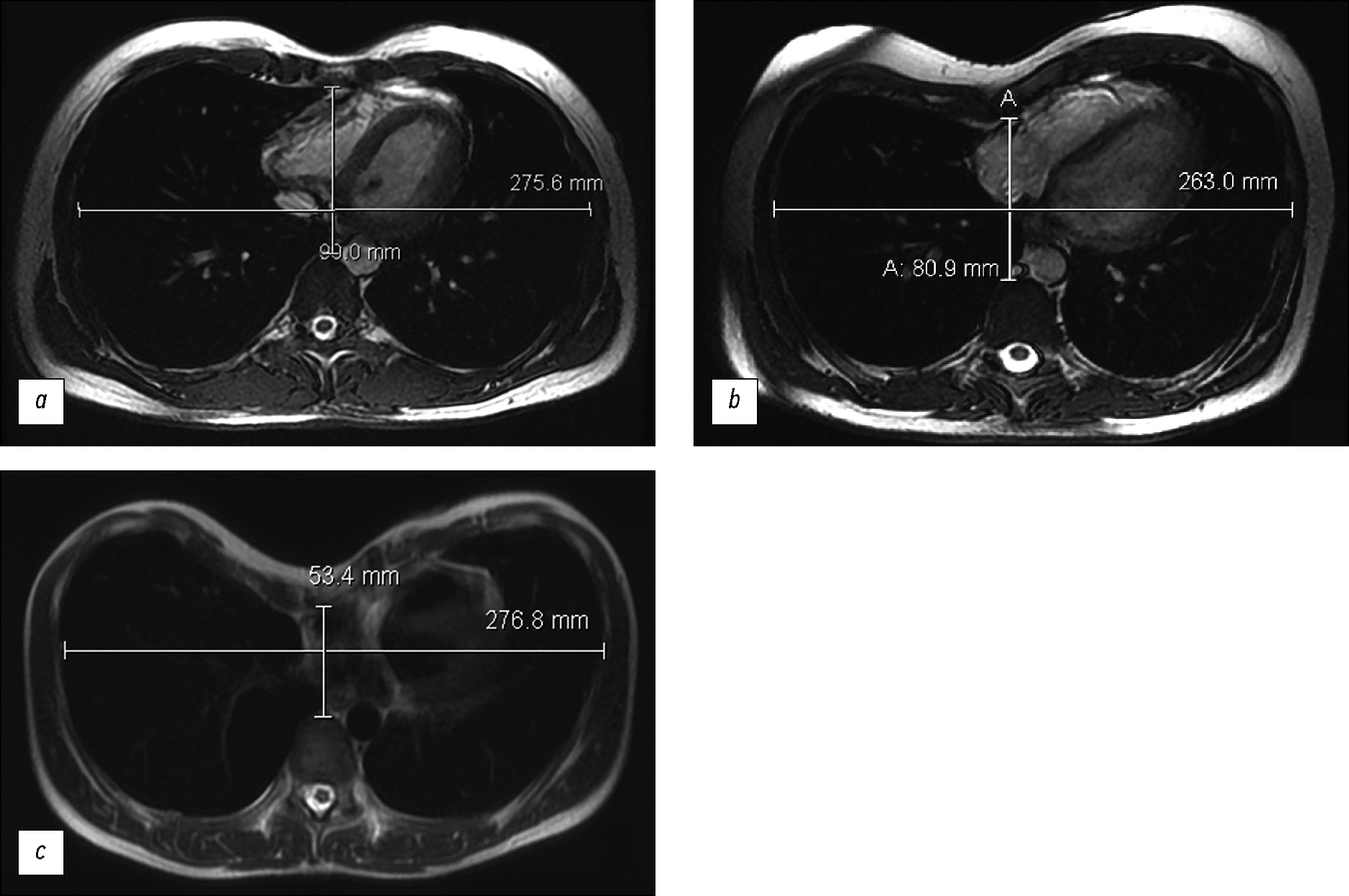
我们根据Haller指数的严重程度将患者分为3个亚组(图1,表1)。轻度 漏斗状胸部畸形患者不再接受手术治疗。中度和重度胸廓畸形患者接受畸形矫正。

图 1. 最大畸形处胸部器官的磁共振成像:a — Haller 指数 3.1;b — Haller 指数 3.3;c — Haller 指数 5.2。
表 1. 按 Haller 指数值分列的患者分布情况
漏斗状胸部畸形 | |||
软质 | 中度 | 重型 | |
患者人数 | 3 | 6 | 29 |
Haller 指数的平均值 | 2.8 | 3.3 | 5.1 |
Haller 指数的标准偏差 | 0.4 | 0.1 | 1.8 |
当搜索Haller指数的值与右心室射血分数之间的关系时,没有获得统计学上显着的Pearson相关 性(吸气射血分数值p=0.777,呼气射血分数值p=0.798)(图2,表2)。右心室射血分数的平均值为46%。

图 2. 显示所研究参数之间是否存在关系。SA:胸骨旋转角度;RVEF:右心室射血分数。
表 2. 呼气和呼气时变量值(Haller 指数和胸骨旋转角度)与右心室射血分数的关系
可变 | 更正指数 | 右心室射血分数 | |
吸气 | 呼气 | ||
胸骨旋转角度 | R=0.19 p=0.255 | R=0.18 p=0.306 | R=0 p=0.99 |
Haller 指数 | R=0.7 p <0.001 | R=–0.05 p=0.777 | R=–0.04 p=0.798 |
Haller指数与胸骨旋转角度之间没有统计学显着关系(p=0.9489)。
矫正指数
在我们的研究中,矫正指数的平均值为 31.5(±11)(图 3)。在统计分析中,随着Haller指数的增加(胸部器官畸形程度的增加),矫正指数也随之增加,P < 0.05(图 4)。因此,轻度 漏斗状胸部畸形患者的矫正指数平均值为 13,中度和重度畸形患者的矫正指数平均值分别为 24 和 35。

图 3. 最大畸形处胸部器官的磁共振成像:a — 矫正指数为 7%;b — 矫正指数为 32%。

图 4. 显示 Haller 与校正指数值之间的相关性(P <0.05)。
胸骨旋转角度与矫正指数之间(P=0.35)以及矫正指数与右心室射血分数之间(P=0.1)均无统计学意义。
胸骨旋转角度
胸骨旋转角度是决定治疗策略的一个重要因素(图 5)。

图 5. 最大畸形处胸部器官的磁共振成像:a — 胸骨旋转角度为 14.3°;b — 胸骨旋转角度为 31.1°。
在44.7%的患者中,角度≥150对手术干预具有重要意义(表3)。这种胸骨位置需要矫正板的非标准倾斜安装。该位置是“朝向”胸骨的锐角进行的,目的是随后将其翻转。因此,如果锐角指向右侧,则矫正钢板应从右侧肋骨上间隙穿过胸骨旋转畸形的峰值,放置到左侧肋骨下间隙(图6,a)。这种旋转占所有胸骨旋转病例的86%。在左侧锐角的病例 中(占所有病例的14%),矫正钢板从右侧的下肋间隙穿过畸形的峰值,放置到左侧的上肋间 隙(图6,b)。
表3。 胸骨旋转角度值对患者的分布
胸骨旋转角度 <15° | |
患者人数 | 21 |
平均角度值 | 10° |
胸骨旋转角度>15° | |
患者人数 | 17 |
平均角度值 | 26° |

图 6. 胸部漏斗畸形矫正后胸部器官的正面投影射线检查。平板在角度方向上的位置:a — 向右;b — 向左。
讨论
传统上,计算机断层扫描一直被用于诊断和分析 漏斗状胸部畸形的参数,由于其普遍性和更容易获得,该方法被广泛使用用[11]。胸部 X 射线计算机断层扫描的明显缺点是存在辐射暴露,而过去几年对扫描方案的修改就是为了减少辐射暴露[12]。
磁共振成像 方法在 漏斗状胸部畸形诊断中并不常见,而且需要更多时间,但其优点是没有辐射照射,而且可以评估心脏压迫变化。
在有针对性地评估 漏斗状胸部畸形时,世界文献中使用了多种指数。其中最常用的是 Haller 指数,该指数用于区分需要手术矫正畸形的患者。该指数的阈值为 3.25。然而,迄今为止,有论文显示,在计划手术干预时,仅使用 Haller 指数可能存在问题。因此,Haller 指数与年龄、手术治疗的其他参数以及术后可能出现的并发症无关[13]。此外,一项对对照组患者和 漏斗状胸部畸形患者的 Haller 指数进行评估的研究显示,两组患者中有 48% 的病例数值相同(数值结果重叠)[9]。
这些结果表明,有必要对数据进行标准化处理,并引入更多指标用于术前和术后评估[9, 13, 14]。一个类似的指数是校正指数,超过该值28%以上是手术指征,前提是与Haller指数相关[15]。校正指数也可用于与术后结果进行比较。
我们的研究得出的 Haller 指数、矫正和胸骨旋转角度值符合患者的临床情况,也符合世界文献中通过计算机断层扫描和 磁共振成像对胸廓畸形进行术前评估的数据[16, 17]。
在我们的研究中,漏斗状胸部畸形患者的右心室射血分数平均值降低至 46%。这些结果与文献数据一致,即变形会导致右心室射血分数降低[18-20]。然而,统计分析并未显示盖勒指数数值与射血分数之间存在相关性,这可能是由于患者根据畸形程度的严重程度分布不均造成的,需要进一步研究。
研究局限性
我们研究的局限性包括其回顾性、患者样本量相对较小、患者在变化增加程度方面的分布不均匀,以及缺乏与金标准--胸部器官计算机断层扫描--的比较。
结论
我们的研究表明,磁共振成像是一种对 漏斗状胸部畸形有高度参考价值的诊断方法,且无辐射负担,还能对病理变化进行详细的术前评估。
有证据表明,Haller 和校正指数值之间存在相关性(P<0.05)。
在我们的研究中,漏斗状胸部畸形患者的特点是右心室射血分数降低。然而,数值与Haller指数并不相关,这可能是由于研究的局限性造成的。
ADDITIONAL INFORMATION
Funding source. This study was not supported by any external sources of funding.
Competing interests. The authors declare that they have no competing interests.
Authors’ contribution. All authors made a substantial contribution to the conception of the work, acquisition, analysis, interpretation of data for the work, drafting and revising the work, final approval of the version to be published and agree to be accountable for all aspects of the work. M.V. Vishnyakova — study concept and design, text editing; G.S. Muzafarova — writing text, collecting and processing materials; A.S. Abramenko — collection and processing of materials; V.A. Kuzmichev, V.V Gatsutsyn — research concept, text editing.
作者简介
Gulishe S. Muzafarova
Moscow Regional Research and Clinical Institute
Email: gms0495@mail.ru
ORCID iD: 0000-0003-0940-3247
SPIN 代码: 2950-5431
俄罗斯联邦, Moscow
Marina V. Vishnyakova
Moscow Regional Research and Clinical Institute
编辑信件的主要联系方式.
Email: cherridra@mail.ru
ORCID iD: 0000-0003-3838-636X
SPIN 代码: 1137-2991
MD, Dr. Sci. (Medicine)
俄罗斯联邦, MoscowAlexander S. Abramenko
Moscow Regional Research and Clinical Institute
Email: a.s.abramenko@gmail.com
ORCID iD: 0000-0002-6286-2162
SPIN 代码: 9743-3001
俄罗斯联邦, Moscow
Vladimir A. Kuzmichev
Moscow Regional Research and Clinical Institute
Email: vakuzmichev@gmail.ru
ORCID iD: 0000-0001-6493-8012
SPIN 代码: 8345-5298
MD, Cand. Sci. (Medicine), Professor
俄罗斯联邦, MoscowVladimir V. Gatsutsyn
Moscow Regional Research and Clinical Institute
Email: vg86@list.ru
ORCID iD: 0000-0002-2364-5325
SPIN 代码: 1431-4417
俄罗斯联邦, Moscow
参考
- Pechetov AA, Esakov JuS, Gubajdullina GF, Makov MA, Hlan’ TN. Differetial approach for chest wall reconstruction for pectus excavatum for adult. N.I. Pirogov Journal of Surgery. 2017;(7):24–29. doi: 10.17116/hirurgia2017724-29
- Fokin АА, Steuerwald NM, Ahrens WA, Allen KE. Anatomical, histologic, and genetic characteristics of congenital chest wall deformities. Seminars in Thoracic and Cardiovascular Surgery. 2009;21(1):44–57. doi: 10.1053/j.semtcvs.2009.03.001
- Scalise PN, Demehri FR. The management of pectus excavatum in pediatric patients: a narrative review. Transl Pediatr. 2023;12(2):208–220. doi: 10.21037/tp-22-361
- Trò R, Martini S, Stagnaro N, et al. A new tool for assessing Pectus Excavatum by a semi-automatic image processing pipeline calculating the classical severity indexes and a new marker: the Volumetric Correction Index. BMC Med Imaging. 2022. doi: 10.1186/s12880-022-00754-0
- Andreyev PS, Skvortsov AP, Tsoy IV, et al. Treatment of funnel breast in children and adolescents. Practical medicine. 2021;19(4):138–141. doi: 10.32000/2072-1757-2021-4-138-141
- Andreev PS, Skvortsov AР, Khabibyanov RYa, Maleev MV. Our experience in surgical treatment of penetral chest deformation. Annali d’Italia. 2023;(41):53–57. doi: 10.5281/zenodo.7774296
- Haller JA Jr, Kramer SS, Lietman SA, et al. Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg. 1987;22(10):904–906. doi: 10.1016/s0022-3468(87)80585-7
- Sidden CR, Katz ME, Swoveland BC, Nuss D. Radiologic considerations in patients undergoing the Nuss procedure for correction of pectus excavatum. Pediatric Radiology. 2001;31(6):429–434. doi: 10.1007/s002470100455
- St. Peter SD, Juang D, Garey CL, et al. A novel measure for pectus excavatum: the correction index. Journal of Pediatric Surgery. 2011;46(12):2270–2273. doi: 10.1016/j.jpedsurg.2011.09.009
- Tauchi R, Suzuki Y, Tsuji T, et al. Clinical Characteristics and Thoracic factors in patients with Idiopathic and Syndromic Scoliosis Associated with Pectus Excavatum. Spine Surg Relat Res. 2018;2(1):37–41. doi: 10.22603/ssrr.2017-0027
- Shamsiev AM, Shamsiev ZhA, Turaev JuA, Mutalibov AI, Burgutov MZh. The role of functional studies of the cardiorespiratory system with funnel chest deformity. Journal Problems of Biology and Medicine. 2017;1(93):9–14.
- Peng R, Mardakhaev E, Shmukler A, Levsky JM, Haramati LB. Meeting ACR Dose Guidelines for CT Lung Cancer Screening in an Overweight and Obese Population. Acad Radiol. 2021;28(3):381–386. doi: 10.1016/j.acra.2020.02.009
- Mortellaro VE, Iqbal CW, Fike FB, et al. The predictive value of Haller index in patients undergoing pectus bar repair for pectus excavatum. J Surg Res. 2011;170(1):104–106. doi: 10.1016/j.jss.2011.02.014
- Karakılıç A, Karaçam V, Ersöz H, et al. Determination of severity of deformity with rib length to costal cartilage length ratio in thorax deformities. Turk Gogus Kalp Damar Cerrahisi Derg. 2018;26(2):279–285. doi: 10.5606/tgkdc.dergisi.2018.15009
- Poston PM, Patel SS, Rajput M, et al. The correction index: setting the standard for recommending operative repair of pectus excavatum. Ann Thorac Surg. 2014;97(4):1176–1180. doi: 10.1016/j.athoracsur.2013.12.050
- Marcovici PA, LoSasso BE, Kruk P, Dwek JR. MRI for the evaluation of pectus excavatum. Pediatric Radiology. 2011;41:757–758. doi: 10.1007/s00247-011-2031-5
- Lollert A, Funk J, Tietze N, et al. Morphologic assessment of thoracic deformities for the preoperative evaluation of pectus excavatum by magnetic resonance imaging. European Radiology. 2015;25:785–791. doi: 10.1007/s00330-014-3450-0
- Dore M, Triana JP, Bret M, et al. Advantages of Cardiac Magnetic Resonance Imaging for Severe Pectus Excavatum Assessment in Children. Eur J Pediatr Surg. 2018;28(1):34–38. doi: 10.1055/s-0037-1604427
- Saleh RS, Finn JP, Fenchel M, et al. Cardiovascular magnetic resonance in patients with pectus excavatum compared with normal controls. J Cardiovasc Magn Reson. 2010;12(1). doi: 10.1186/1532-429X-12-73
- Stagnaro N, Trocchio G, Torre M, et al. Cardiovascular MRI assessment of pectus excavatum in pediatric patients and postoperative simulation using vacuum bell. J Pediatr Surg. 2021;56(9):1600–1605. doi: 10.1016/j.jpedsurg.2020.11.017
补充文件



